
Alejandro González Veliz: Not Every Acs Patient Needs 12 Months of Dapt
Alejandro González Veliz, Interventional Cardiologist at Institute of Cardiology and Cardiovascular Surgery, shared a post on LinkedIn about a recent article by Diana A. Gorog et al., published in Euro Intervention, adding:
“Not Every Acs Patient Needs 12 Months of Dapt.
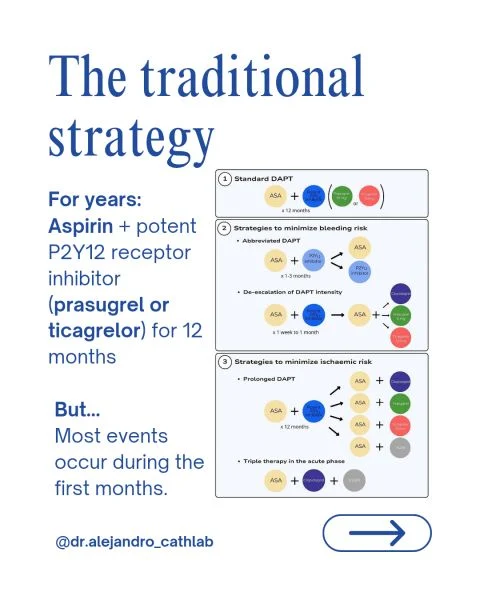
For years, the standard approach after ACS treated with PCI was simple:
Aspirin plus a potent P2Y12 inhibitor
For 12 months
But cardiology is evolving.
The new ESC Clinical Consensus reminds us that antiplatelet therapy should not be a ‘one-size-fits-all’ strategy anymore.
The real challenge is balancing:
- Ischemic risk
- Bleeding risk
And surprisingly…
Bleeding risk is often More common than high ischemic risk.
Why is this important?
Because major bleeding is not a minor complication.
It is associated with:
- Higher mortality
- More hospitalizations
- Treatment discontinuation
- Worse long-term outcomes
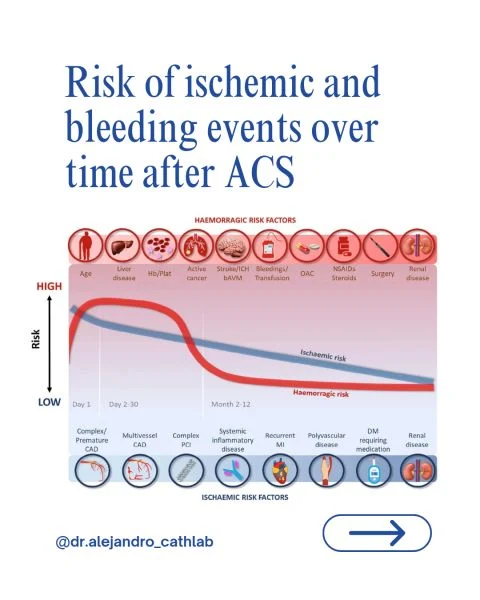
Meanwhile, with modern drug-eluting stents:
- Stent thrombosis is uncommon
- Most ischemic events occur early
- Risk decreases substantially after the first months
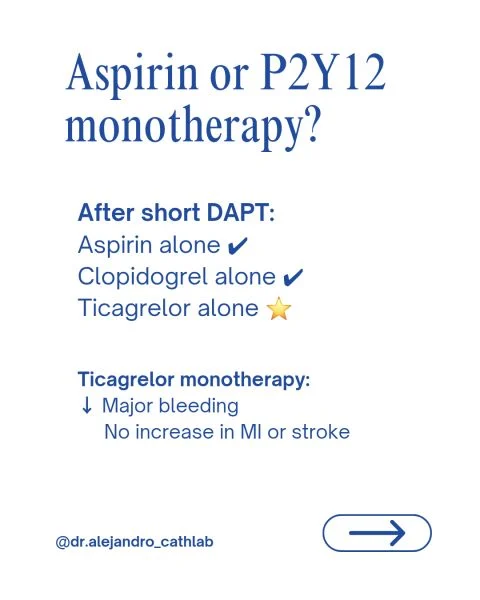
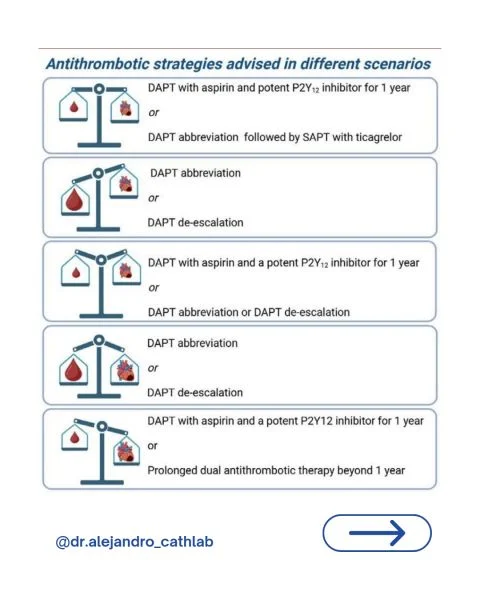
This has opened the door to new strategies:
- Shorter DAPT duration
- P2Y12 inhibitor monotherapy
- DAPT de-escalation
- Extended therapy only for selected high ischemic-risk patients
But shorter is not always better.
The message of this consensus is clear:
- Assess the patient.
- Identify bleeding risk.
- Identify ischemic risk.
- Individualize treatment.
Because the best antiplatelet strategy is not necessarily the most aggressive…
It’s the one that provides the best balance between efficacy and safety.
Key take-home messages:
- Standard DAPT remains the default strategy.
- Bleeding risk is more prevalent than ischemic risk.
- Short DAPT followed by monotherapy is effective in selected patients.
- Ticagrelor monotherapy is among the strongest alternatives after abbreviated DAPT.
- Antiplatelet therapy after ACS should be personalized, not standardized.
- Treat the patient. Not the protocol.
EuroIntervention 2026”
Title:Antithrombotic therapy for secondary prevention in patients with acute coronary syndromes treated with percutaneous coronary intervention: options for personalization to reduce bleeding or ischaemic risks
Authors: Diana A. Gorog, Jurriën M. ten Berg, Gianluca Campo, Tobias Geisler, Bruna Gigante, Erik L. Grove, Sigrun Halvorsen, Kurt Huber, Young-Hoon Jeong, Gregory Y. H. Lip, Eliano P. Navarese, Andrea Rubboli, Jolanta M. Siller Matula, Robert F. Storey, Marco Valgimigli, Christophe Vandenbriele, Gemma Vilahur, Ingo Ahrens, Jose Luis Ferreiro

Other posts featuring Alejandro González Veliz on Hemostasis Today.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-
Aug 4, 2026, 07:12Nikolaos Evangelidis: Optimizing Blood Pressure Control in Everyday Practice
-
Aug 4, 2026, 07:09Mohsen Sedighi: Inflammatory Biomarkers as Predictors of Acute Stroke in Hospitalized COVID-19 Patients
-
Aug 4, 2026, 07:07Gemma Figtree: Using Ultra-Low Troponin Levels to Guide Coronary CT Scans
-
Aug 4, 2026, 07:06Rucha Patil: Advancing Haemostasis Through Science, Collaboration and Innovation at NHU 2026
-
Aug 4, 2026, 07:01Wolfgang Miesbach: Factor VIII Aurora Redefines the Biology of Coagulation
-
Aug 4, 2026, 06:51Katrina Snow: Choosing Wisely in Transfusion Medicine
-
Aug 4, 2026, 06:37Pall T. Onundarson: Is PT/INR the Problem, Not Warfarin?
-
Aug 4, 2026, 06:30Kriti Batni: Strengthening Pediatric Hemovigilance in Transfusion Medicine
-
Aug 4, 2026, 06:28Alejandro González Veliz: Not All Calories Are Created Equal