
AI Generated
Apr 21, 2026, 14:36
Chokri Ben Lamine: 50 Pearls Credits on How is Breakthrough Thrombosis in Patients with Cancer Being Treated
Chokri Ben Lamine, Adult Hematology and SCT Assistant Consultant at Oncology Center of Excellence at King Faisal Specialist Hospital and Research Center, shared a post on X:
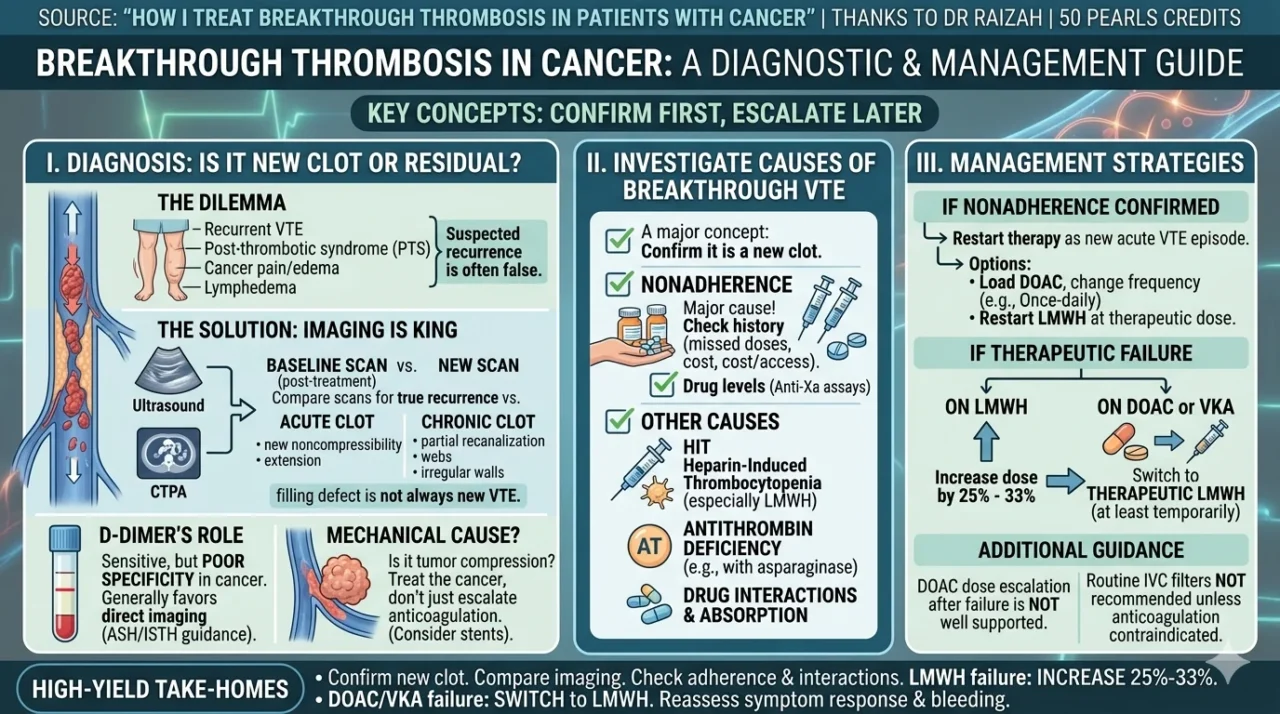
“Breakthrough thrombosis in cancer:
50 pearls Credits for sharing to Dr Raizah
Source: How I treat breakthrough thrombosis in patients with cancer
- Breakthrough VTE in cancer is not rare despite anticoagulation.
- Reported 6-month cumulative incidence is ~5%–8%.
- In cancer, recurrence on treatment is more common than in non-cancer patients.
- Before changing treatment, first ask: Is this true recurrence or residual old clot?
- Only about one-quarter of suspected recurrent VTE cases are objectively confirmed.
- Post-thrombotic syndrome can mimic recurrent DVT.
- Post-PE syndrome can mimic recurrent PE.
- Cancer-related pain, swelling, dyspnea, edema, and lymphedema can all confuse the picture.
- The most important diagnostic step is careful imaging review.
- Best practice: compare with a postindex baseline scan done after initial treatment.
- Residual thrombus is very common after treated DVT.
- At ~6 months, many patients still have residual venous obstruction.
- In cancer, residual abnormalities can persist even more often than in non-cancer patients.
- After PE, residual radiologic changes may still be present up to 1 year later.
- So a ‘filling defect’ on imaging is not automatically new VTE.
- Acute recurrent DVT is suggested by new noncompressibility of a previously compressible segment.
- Increase in residual thrombus diameter may support recurrence, but measurements have interobserver variability.
- Acute PE is suggested by new intraluminal filling defects or extension of prior defects.
- Features such as partial recanalization, thin webs, irregular wall thickening favor chronic clot.
- If imaging looks chronic and no baseline exists, a reasonable approach can be repeat ultrasound in 7–10 days rather than immediate escalation.
- A major concept: confirm first, escalate later.
- In suspected breakthrough VTE, D-dimer is not very helpful in most cancer patients.
- Why? Cancer plus prior VTE already push pretest probability upward.
- D-dimer remains sensitive, but specificity is poor in cancer.
- ASH/ISTH guidance generally favors direct imaging over D-dimer in this setting.
- If tumor is causing extrinsic venous compression, the issue may be mechanical, not purely hypercoagulable.
- In mechanical compression, treating the cancer may be more important than simply escalating anticoagulation.
- Selected symptomatic cases may need interventional options like venous stenting.
- Always ask whether symptoms are driven by mixed pathology: clot plus tumor plus lymphatic obstruction.
- Baseline imaging after ~6 months of anticoagulation is an excellent practical habit in cancer-associated thrombosis.
- Once true breakthrough thrombosis is confirmed, first assess adherence.
- Nonadherence is a major and common reason for apparent treatment failure.
- Take a detailed medication history: missed doses, wrong timing, self-held doses, cost/access issues.
- Drug levels can sometimes help confirm nonadherence when history is unclear.
- For DOACs and LMWH, anti-Xa assays may show whether meaningful drug exposure is present.
- A negative anti-Xa near the expected window strongly suggests little or no anticoagulant effect.
- If nonadherence is confirmed, manage as a new acute VTE episode.
- For DOAC restart, use the appropriate loading regimen when indicated.
- If twice-daily adherence is poor, a once-daily option may sometimes be more practical.
- If LMWH is chosen after nonadherence, restart at full weight-based therapeutic dose.
- In patients on LMWH, think about HIT if thrombosis occurs with new thrombocytopenia or platelet drop.
- HIT is uncommon with LMWH, but it is important because it is prothrombotic.
- Also think of acquired antithrombin deficiency, especially with asparaginase exposure.
- Antithrombin deficiency can lead to subtherapeutic heparin effect.
- In confirmed breakthrough VTE on therapeutic LMWH, most guidance supports increasing LMWH by 25%–33%.
- In breakthrough VTE on subtherapeutic LMWH, increase to full therapeutic weight-adjusted dose.
- In breakthrough VTE on a DOAC or VKA, current practice generally favors switching to therapeutic LMWH, at least temporarily.
- Routine switch from LMWH to DOAC after LMWH failure is not well supported by current data.
- DOAC dose escalation after DOAC failure is not supported by good evidence.
- IVC filters are not recommended routinely unless anticoagulation is contraindicated.
High-yield take-home
- Confirm it is new clot.
- Compare with old imaging whenever possible.
- Check adherence, interactions, absorption, HIT, antithrombin deficiency, mechanical compression.
- LMWH failure – increase.
- LMWH 25%–33% DOAC/VKA failure – switch to therapeutic LMWH.
- Reassess early for symptom response and bleeding.”

More posts featuring Chokri Ben Lamine on Hemostasis Today.
-
Jul 28, 2026, 07:10Wolfgang Miesbach: How Safe Is AAV Gene Therapy?
-
Jul 28, 2026, 06:59Fiona Robinson: New MASAC Recommendations for Iron Deficiency – Live Webinar
-
Jul 28, 2026, 06:49Vera Ghali: What Else Do Platelets Do Besides Clotting?
-
Jul 28, 2026, 02:54Joseph R. Shaw: Why Stroke Occurs Despite Anticoagulation
-
Jul 28, 2026, 02:45Are VWD Clinical Trials Missing What Matters Most to Women? – RPTH
-
Jul 28, 2026, 02:38Umberto Pensato: New BMJ Review on Breakthrough Stroke in Patients Receiving DOACs Is Now Live
-
Jul 27, 2026, 17:29Muhammad Numan: Normal MCV Does Not Exclude B12 Deficiency
-
Jul 27, 2026, 17:15ISTH 2026 Congress Paris Opens with a Powerful Message: Science Beyond Border
-
Jul 27, 2026, 17:14Michael Ombrello։ Decoding How Autoantibodies Cause Disease