
Chokri Ben Lamine: Clinical Insights into Glanzmann Thrombasthenia and Heavy Menstrual Bleeding
Chokri Ben Lamine, Adult Hematology and SCT Assistant Consultant at Oncology Center of Excellence at King Faisal Specialist Hospital and Research Center, shared a post on X:
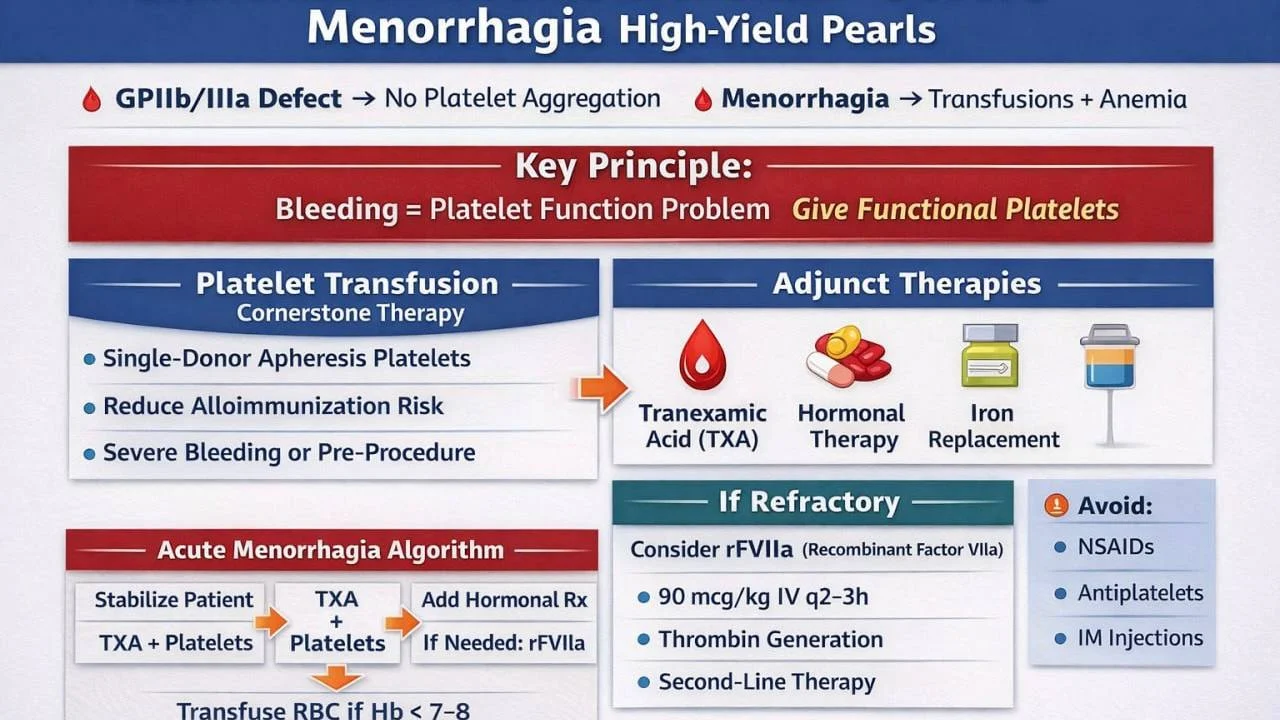
”Glanzmann Thrombasthenia and Severe Menorrhagia – High-Yield Pearls
Glanzmann thrombasthenia (GT) is caused by defect in GPIIb/IIIa (αIIbβ3)
Platelet count normal but aggregation absent resulting in severe mucosal bleeding
Menorrhagia is a major morbidity driver in GT
It leads to recurrent transfusion requirements iron deficiency anemia
Key principle:
- Bleeding is a platelet function problem and give functional platelets
- Platlet transfusion is the cornerstone of therapy in severe bleeding
Rationale:
- GT platelets lack GPIIb/IIIa
- Transfused normal donor platelets restore aggregation
- Provide functional fibrinogen bridging, resulting in a stable clot
This is pathophysiologically targeted therapy
Indication for platelets:
- Severe menorrhagia (Hb drop / hemodynamic impact)
- Active uncontrolled bleeding
- Pre-procedure
Preferred product:
- Single-donor apheresis platelets
- Reduce alloimmunization risk
Major limitation:
Alloimmunization to:
- HLA antigens
- GPIIb/IIIa
Consequence:
- Platelet refractoriness leads to reduced efficacy
Therefore:
- Use platelets judiciously but early when indicated
Adjunct therapy (always combine):
Tranexamic acid (TXA)
- Stabilizes clot
- Dose: 1–1.5 g PO/IV q8h
Hormonal therapy
- Combined OCPs or progesterone
- Decreased endometrial shedding
Iron replacement
- Oral or IV
If platelet refractoriness OR antibodies present:
- rFVIIa (NovoSeven® – eptacog alfa)
Dose:
- 90 µg/kg IV q2–3h
Mechanism:
- Generates thrombin independent of platelet aggregation
rFVIIa is second-line therapy, not first-line.
Avoid overusing rFVIIa early if platelets still effective
Acute severe menorrhagia algorithm:
- Stabilize patient with IV fluids, with or without RBC transfusion.
- Start TXA immediately
- Give platelet transfusion early
- Add hormonal therapy
- If refractory, give rFVIIa.
Transfusion thresholds:
- Hemoglobin less than 7–8 or symptomatic leads to RBC transfusion
Avoid:
- NSAIDs
- Antiplatelets
- IM injections
Long-term prevention:
- Continuous OCPs
- LNG-IUS (Mirena® – levonorgestrel IUD)
- Cyclic TXA during menses
Goal:
- Minimize need for platelet transfusions
Special situations:
- Adolescents require early hormonal control
Pregnancy requires MDT (hematology plus OB)
Pre-procedure:
- Platelets with or without TXA with or without rFVIIa depending on severity
Key clinical insight:
- Platelets treat the defect, whereas rFVIIa bypasses it
Always prioritize platelet transfusion FIRST in severe bleeding
Preserve platelet efficacy by avoiding unnecessary exposure.
Use combined mechanistic and supportive therapy.
OSCE Scenario:
- 20F GT, Hb 6.8, ongoing heavy bleeding
- TXA plus RBC transfusion and apheresis platelets FIRST
- If poor response, rFVIIa
MCQ:
First-line therapy in severe GT menorrhagia (no antibodies)?
- rFVIIa
- TXA alone
- Platelet transfusion
- Warfarin
Answer: C – replaces defective platelet function.”
More posts featuring Chokri Ben Lamine on Hemostasis Today.
-
Jul 28, 2026, 02:54Joseph R. Shaw: Why Stroke Occurs Despite Anticoagulation
-
Jul 28, 2026, 02:45Are VWD Clinical Trials Missing What Matters Most to Women? – RPTH
-
Jul 28, 2026, 02:38Umberto Pensato: New BMJ Review on Breakthrough Stroke in Patients Receiving DOACs Is Now Live
-
Jul 27, 2026, 17:29Muhammad Numan: Normal MCV Does Not Exclude B12 Deficiency
-
Jul 27, 2026, 17:15ISTH 2026 Congress Paris Opens with a Powerful Message: Science Beyond Border
-
Jul 27, 2026, 17:14Michael Ombrello։ Decoding How Autoantibodies Cause Disease
-
Jul 27, 2026, 16:57Thomas Dayspring։ Could PCSK9 Inhibitors Reduce the Risk of Retinal Vascular Occlusions?
-
Jul 27, 2026, 16:53Arun V. J.: How to Find a Mentor When You Know No One
-
Jul 27, 2026, 16:45Urtė Cholinaitė: A Meaningful Experience at the Lithuania Hemophilia Society Summer Camp