
Chokri Ben Lamine: High-Yield Pearls from a Heme Perspective on Uremic Coagulopathy
Chokri Ben Lamine, Assistant Consultant at King Faisal Specialist Hospital and Research Center, shared a post on X:
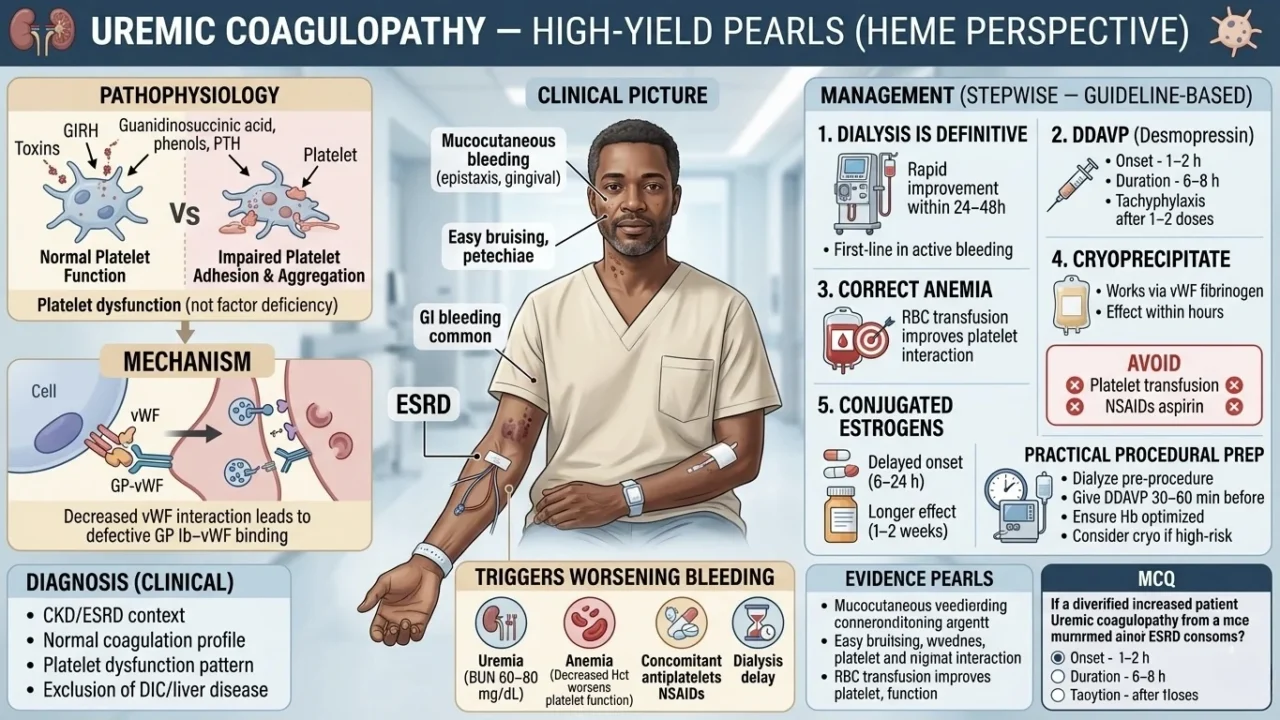
“Uremic Coagulopathy — High-Yield Pearls (Heme Perspective)
- Pathophysiology is platelet dysfunction (not factor deficiency)
- Mechanism is impaired platelet adhesion with aggregation
- Key toxins include guanidinosuccinic acid, phenols, PTH
- Decreased vWF interaction leads to defective GP Ib–vWF binding
- Platelet count is usually normal
- PT/PTT is usually normal
- Bleeding time and PFA-100 is prolonged
Clinical picture
- Mucocutaneous bleeding (epistaxis, gingival)
- Easy bruising, petechiae
- GI bleeding common
- Increased Post-procedure bleeding risk
Triggers worsening bleeding
- Uremia (BUN 60–80 mg/dL)
- Anemia ( Decreased Hct worsens platelet function)
- Concomitant antiplatelets NSAIDs
- Dialysis delay
Diagnosis (clinical)
- CKD/ESRD context
- Normal coagulation profile
- Platelet dysfunction pattern
- Exclusion of DIC/liver disease
Management (stepwise — guideline-based)
1.Dialysis is definitive
- Rapid improvement within 24–48h
- First-line in active bleeding
2.DDAVP (Desmopressin)
- 0.3 mcg/kg IV over 20–30 min
- Onset – 1–2 h
- Duration – 6–8 h
- Tachyphylaxis after 1–2 doses
3.Correct anemia
- Target Hb 10 g/dL
- RBC transfusion improves platelet interaction
4.Cryoprecipitate
- If bleeding persists
- Works via vWF fibrinogen
- Effect within hours
5.Conjugated estrogens
- 0.6 mg/kg IV daily 5 days
- Delayed onset (6–24 h)
- Longer effect (1–2 weeks)
Avoid
- Platelet transfusion (limited role unless thrombocytopenia)
- NSAIDs aspirin
Practical procedural prep
- Dialyze pre-procedure
- Give DDAVP 30–60 min before
- Ensure Hb optimized
- Consider cryo if high-risk
Evidence pearls
- DDAVP is transient but effective (standard of care for urgent bleeding)
- Dialysis is cornerstone (KDIGO CKD guidelines)
- Estrogens are useful in recurrent bleeding when dialysis insufficient
MCQ
Patient with ESRD and epistaxis and normal PT and PTT:
What is the best immediate therapy?
- FFP
- Platelets
- DDAVP
- Vitamin K
Answer:
C (DDAVP) — fastest hemostatic correction
OSCE scenario
ESRD patient needs central line
Plan:
Perform dialysis, then administer DDAVP pre-procedure, optimize hemoglobin, and avoid NSAIDs”
Other posts featuring Chokri Ben Lamine on Hemostasis Today.
-
Aug 11, 2026, 07:50When Access to Care Changes Everything – WFH
-
Aug 11, 2026, 07:41Kevin Land: How Cellular Therapy Is Changing Transfusion Medicine
-
Aug 11, 2026, 07:35Kuldeep Singh Bhadauria: Building the Future of Hemophilia Care in India
-
Aug 11, 2026, 07:28Archil Jaliashvili: When Every Minute Matters Time Becomes a Therapy
-
Aug 11, 2026, 07:05Mavis Agnes Kisakye: Building Sustainable Transition Pathways in Hemophilia Care
-
Aug 11, 2026, 06:48Rishdha Roshad: What Happens to the Brain During Cardiopulmonary Bypass?
-
Aug 11, 2026, 05:53Isaac Okello: Strengthening Sickle Cell Advocacy in Uganda
-
Aug 11, 2026, 05:38Rami Unterman: A Simple New Biomarker for Fibrotic ILDs
-
Aug 11, 2026, 04:10Haroun Gajraj: CLaCS vs Sclerotherapy – What Does the Evidence Show