
Aynetu Girma Moges: Major Cardiovascular Changes in Pregnancy
Aynetu Girma Moges, Humanitarian Aid Worker in SRH and GBV at the Ethiopian Midwives Association, shared a post on LinkedIn:
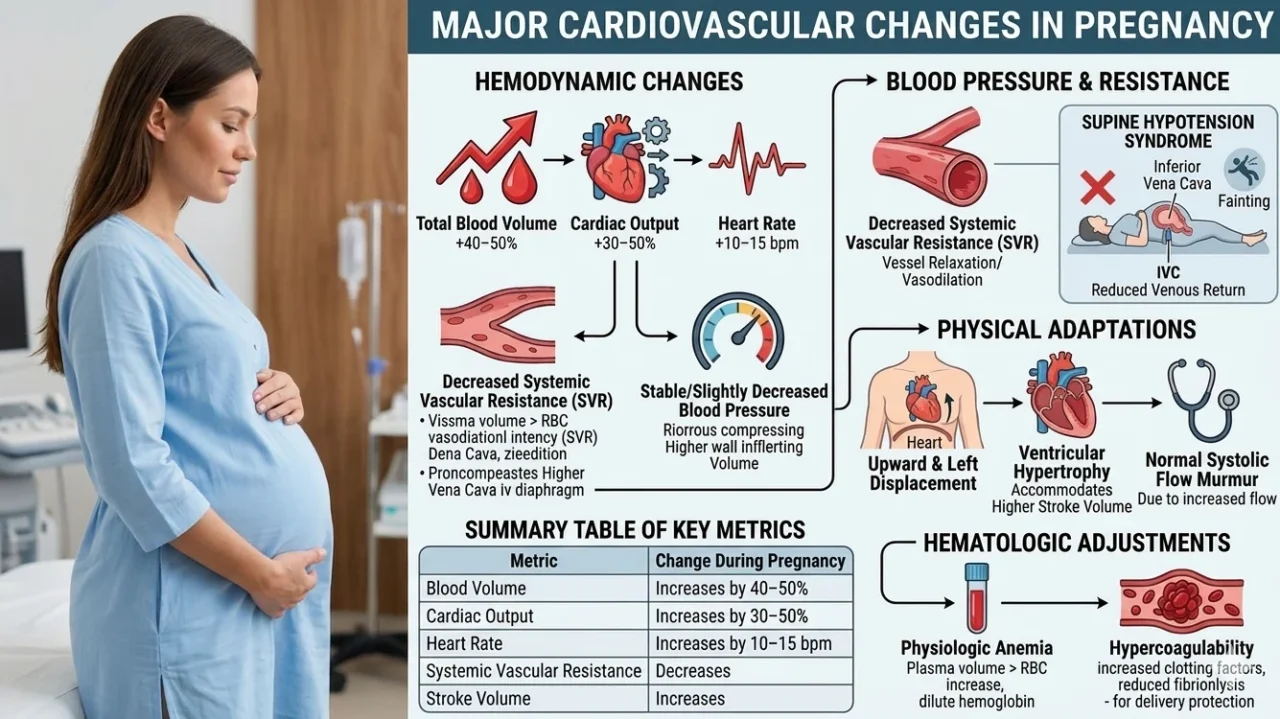
“Cardiovascular Changes (Physiological Adaptation) during Pregnancy
During pregnancy, the cardiovascular system undergoes significant adaptations to meet the increased metabolic demands of both the mother and the developing fetus.
These changes begin as early as five weeks gestation and peak during the second and third trimesters.
1. Hemodynamic changes:
The most notable shifts involve the volume and flow of blood throughout the body.
- Blood Volume Increase: Total blood volume increases by 40% to 50%. This is primarily due to an increase in plasma volume, which helps protect against the blood loss typically experienced during childbirth.
- Cardiac Output: This rises by 30% to 50%. The increase is achieved through a combination of a higher heart rate and a larger stroke volume (the amount of blood pumped with each beat).
- Heart Rate: A gradual increase occurs throughout pregnancy, typically reaching 10 to 15 beats per minute above the pre-pregnancy baseline.
2. Blood pressure and vascular resistance:
Despite the massive increase in blood volume, blood pressure usually remains stable or even decreases slightly due to changes in the blood vessels.
- Systemic Vascular Resistance (SVR): There is a marked decrease in resistance. Progesterone and nitric oxide cause the smooth muscles in the blood vessels to relax (vasodilation), which keeps blood pressure from spiking despite the extra volume.
- Blood Pressure Trends: Systolic and diastolic blood pressure often drop during the second trimester before returning to pre-pregnancy levels near the end of the third trimester.
- Supine Hypotension Syndrome: When lying flat on the back, the heavy uterus can compress the inferior vena cava, reducing blood return to the heart and causing a sudden drop in blood pressure and dizziness.
3. Physical and structural changes
The heart itself adapts physically to the increased workload.
- Heart Displacement: As the uterus grows and pushes the diaphragm upward, the heart is displaced upward and to the left.
- Ventricular Hypertrophy: The heart muscle may slightly enlarge (increase in mass) to accommodate the higher stroke volume, a process that usually reverses after delivery.
- Auscultation Changes: Because of the increased blood flow and heart displacement, it is common (and often normal) to hear a systolic flow murmur during a physical examination.
4. Hematologic adjustments
- Physiologic Anemia: While red blood cell mass increases, the plasma volume increases much more significantly. This ‘dilution’ leads to a lower hemoglobin concentration, often referred to as the physiologic anemia of pregnancy.
- Hypercoagulability: Pregnancy is a ‘pro-thrombotic’ state.”
Stay updated with Hemostasis Today.
-
Jun 1, 2026, 15:24John Chuback: DVT Can Start With Symptoms Many People Brush Off
-
Jun 1, 2026, 15:20Venugopalan Unni: Guidelines for the Evaluation and Management of Acute Pulmonary Embolism in Adults
-
Jun 1, 2026, 15:10Smitirupa Mishra: Standardizing RBC Morphology Reporting – Why ICSH Guidelines Matter?
-
Jun 1, 2026, 14:54Davide Massimi: A Bloodless Approach to Third Space Endoscopy
-
Jun 1, 2026, 14:27Afshan Sumera: Plasma Proteomics Reveals Complement And Coagulation Disruption In Transfusion-Dependent Thalassemia
-
Jun 1, 2026, 13:44Milad Abdalla: Elevating Phlebotomy Standards – Why Order of Draw and Blood Cultures Matter
-
Jun 1, 2026, 13:39Abdul Mannan: The Moral Injury of Practising Haemato-Oncology in a Resource-Limited Setting
-
Jun 1, 2026, 13:34Filza Aslam: What Does a Patient Journey Partner Actually Do in Bleeding Disorders?
-
Jun 1, 2026, 13:33Darine Ghanem: Advancing Health Equity in Care at the LATAM Meeting