
AI Generated
Apr 21, 2026, 15:51
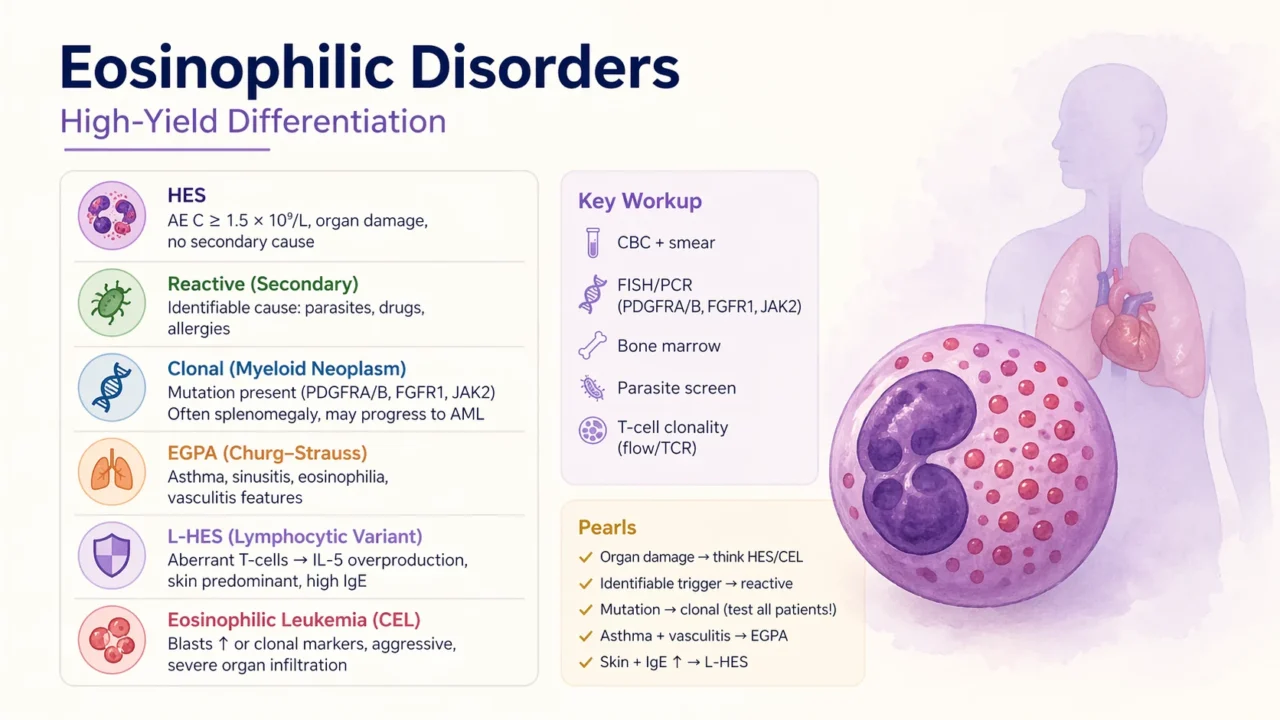
Chokri Ben Lamine: High-Yield Differentiation of Eosinophilic Disorders
Chokri Ben Lamine, Adult Hematology and SCT Assistant Consultant at Oncology Center of Excellence at King Faisal Specialist Hospital and Research Center, shared a post on X:
“Hes vs other eosinophilic disorders – high – yield differentiation
Hypereosinophilic Syndrome (HES)
- AEC greater than or equal to 1.5 multiplied by ten to the power of nine per liter persistently
Organ damage heart skin lungs central nervous system - No secondary cause and no defined clonal malignancy
- Subtypes myeloid for example PDGFRA lymphocytic idiopathic
- Treatment steroids then imatinib if PDGFRA positive then anti interleukin five such as mepolizumab or benralizumab off label
Reactive (Secondary) Eosinophilia
- Cause identified
- Parasites (helminths)
- Drugs (DRESS)
- Allergic diseases (asthma, eczema)
- No primary clonal disorder
- Rx: treat underlying cause
Clonal Eosinophilia Myeloid Neoplasm
- Genetic driver present
- PDGFRA, PDGFRB, FGFR1, PCM1, JAK2
- Often splenomegaly and dysplasia
- Can evolve to acute myeloid leukemia
- Treatment targeted tyrosine kinase inhibitors for example imatinib shows a dramatic response in PDGFRA
EGPA (Churg – Strauss)
- Asthma and sinusitis plus eosinophilia
- Vasculitis features including neuropathy and purpura
- ANCA positive or negative
- Treatment steroids and biologics such as benralizumab or mepolizumab (Food and Drug Administration approved)
Lymphocytic Variant HES (L-HES)
- Aberrant T cells leading to interleukin five overproduction
- Skin predominant disease and high immunoglobulin E
- Risk of T cell lymphoma
- Treatment steroids with or without immunosuppression
Eosinophilic Leukemia (CEL)
- Blasts increased or clonal markers present
- Aggressive clinical course
- Severe organ infiltration
- Treatment leukemia type therapy with or without tyrosine kinase inhibitor
Key Clinical Differentiation Pearls
- Organ damage means consider hypereosinophilic syndrome or eosinophilic leukemia
- Identifiable trigger suggests reactive eosinophilia
- Mutation indicates clonal disease (test all patients)
- Asthma and vasculitis suggests EGPA
- Skin involvement and increased immunoglobulin E suggests lymphocytic variant HES
Workup Snapshot
- Complete blood count and peripheral blood smear
- Fluorescence in situ hybridization and polymerase chain reaction testing for PDGFRA, PDGFRB, FGFR1 and JAK2
- Bone marrow examination
- Parasite screening
- T cell clonality assessment using flow cytometry or T cell receptor studies
MCQ
- Patient with absolute eosinophil count 3.0, asthma, sinusitis, neuropathy leads to best diagnosis
- Answer EGPA (vasculitis plus asthma plus eosinophilia)
OSCE
- Patient with persistent eosinophilia plus cardiac involvement and no secondary cause
- Next step molecular testing for PDGFRA before labeling idiopathic hypereosinophilic syndrome.”
Stay updated with Hemostasis Today.
-
Jul 28, 2026, 02:54Joseph R. Shaw: Why Stroke Occurs Despite Anticoagulation
-
Jul 28, 2026, 02:45Are VWD Clinical Trials Missing What Matters Most to Women? – RPTH
-
Jul 28, 2026, 02:38Umberto Pensato: New BMJ Review on Breakthrough Stroke in Patients Receiving DOACs Is Now Live
-
Jul 27, 2026, 17:29Muhammad Numan: Normal MCV Does Not Exclude B12 Deficiency
-
Jul 27, 2026, 17:15ISTH 2026 Congress Paris Opens with a Powerful Message: Science Beyond Border
-
Jul 27, 2026, 17:14Michael Ombrello։ Decoding How Autoantibodies Cause Disease
-
Jul 27, 2026, 16:57Thomas Dayspring։ Could PCSK9 Inhibitors Reduce the Risk of Retinal Vascular Occlusions?
-
Jul 27, 2026, 16:53Arun V. J.: How to Find a Mentor When You Know No One
-
Jul 27, 2026, 16:45Urtė Cholinaitė: A Meaningful Experience at the Lithuania Hemophilia Society Summer Camp