

Kalyan Roy: Understanding Erythroblastosis Fetalis
Kalyan Roy, Transfusion Medicine Specialist at Square Hospitals LTD, shared a post on LinkedIn:
“Understanding Erythroblastosis Fetalis (Rh Disease)
Erythroblastosis Fetalis, also known as Hemolytic Disease of the Newborn (HDN), is a serious but highly preventable condition where a mother’s immune system attacks her baby’s red blood cells (RBCs).
This immune response leads to fetal anemia and other life-threatening complications.
The Pathophysiology (The Mechanism)
The core of this condition is an isoimmunization process. Here is the step-by-step mechanism:
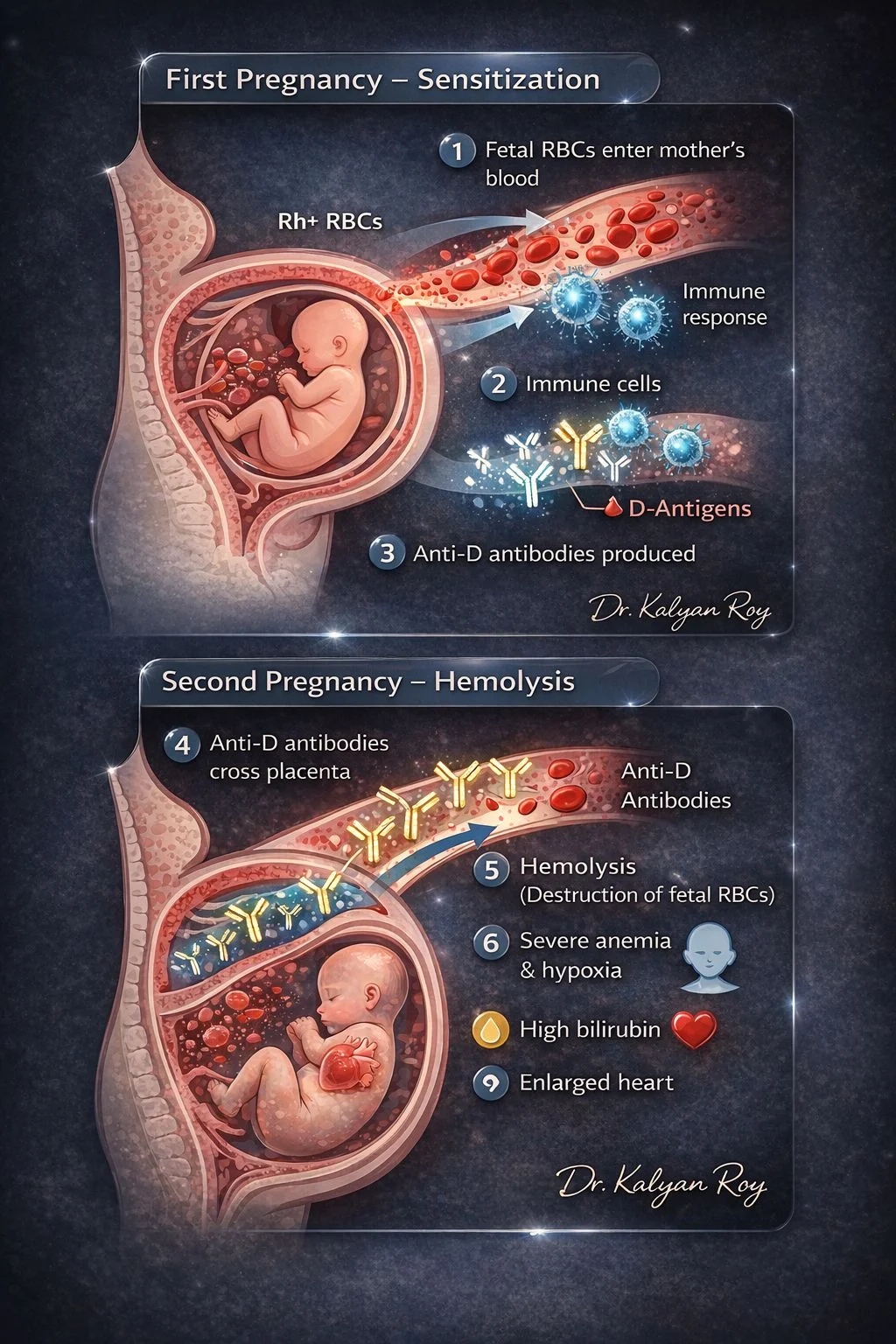
- Maternal Sensitization: When an Rh-negative mother is exposed to Rh-positive fetal RBCs (often during delivery, miscarriage, or trauma), her immune system identifies the ‘D antigen’ as foreign.
- Antibody Production: The mother’s body produces IgG antibodies (anti-D) against these Rh-positive cells.
- Placental Transfer: Unlike other types of antibodies, IgG is small enough to cross the placenta.
- Targeted Destruction: In a subsequent pregnancy with an Rh-positive fetus, these maternal antibodies enter the fetal circulation and bind to the baby’s RBCs.
- Hemolysis: The antibody-coated RBCs are destroyed (hemolysis), leading to a dangerous cycle of anemia and high bilirubin.
How does it happen?
It most commonly occurs due to Rh Incompatibility:
- The Setup: An Rh-negative mother carries an Rh-positive baby.
- The Trigger: Fetal blood enters maternal circulation (e.g., during birth or trauma).
- The Reaction: The mother produces anti-D antibodies.
- The Result: In the next pregnancy, these antibodies cross the placenta and destroy the new baby’s RBCs.
Why is it dangerous?
The destruction of fetal RBCs leads to several critical issues:
- Severe Anaemia: The baby lacks enough oxygen-carrying cells.
- High Bilirubin (Jaundice): RBC breakdown creates bilirubin. If untreated after birth, it can lead to Kernicterus (permanent brain damage).
- Hydrops Fetalis: In severe cases, the anemia leads to heart failure, causing extreme swelling (edema) and fluid accumulation (ascites) in the fetus.
Diagnosis and Management
During Pregnancy:
- Indirect Coombs Test: To check the mother’s blood for antibodies.
- MCA Doppler and Ultrasound: To monitor for signs of fetal anemia or hydrops.
- Intrauterine Transfusion: In severe cases, blood is given to the baby while still in the womb.
After Birth:
- Direct Coombs Test: Performed on the baby’s blood to confirm the presence of maternal antibodies on their RBCs.
- Treatments: Include phototherapy (for jaundice), exchange transfusions, or standard blood transfusions.
Prevention: The Key to Safety
This condition is almost entirely preventable! Rh-negative mothers are given Anti-D Immunoglobulin (e.g., RhoGAM):
At 28 weeks of pregnancy.
Within 72 hours after the delivery of an Rh-positive baby.
Following any miscarriage, abortion, trauma, or invasive prenatal procedure.
Note: The first pregnancy is usually unaffected because the mother hasn’t been sensitized yet.
Prevention is focused on protecting all future babies!”

Stay updated with Hemostasis Today.
{kind=link}
-
Aug 11, 2026, 08:20Hasan Abbas Zaheer: Strengthening Universal Access to Safe Blood in Pakistan
-
Aug 11, 2026, 08:07Nicola Pozzi: Advancing Hemostasis Through Scientific Collaboration at Hemostasis GRC
-
Aug 11, 2026, 07:50When Access to Care Changes Everything – WFH
-
Aug 11, 2026, 07:41Kevin Land: How Cellular Therapy Is Changing Transfusion Medicine
-
Aug 11, 2026, 07:35Kuldeep Singh Bhadauria: Building the Future of Hemophilia Care in India
-
Aug 11, 2026, 07:28Archil Jaliashvili: When Every Minute Matters Time Becomes a Therapy
-
Aug 11, 2026, 07:05Mavis Agnes Kisakye: Building Sustainable Transition Pathways in Hemophilia Care
-
Aug 11, 2026, 06:48Rishdha Roshad: What Happens to the Brain During Cardiopulmonary Bypass?
-
Aug 11, 2026, 05:53Isaac Okello: Strengthening Sickle Cell Advocacy in Uganda