

Rowan Paul: Immune Privilege versus Immune Evasion – Why MSCs Are Not What We Thought
Joe Purita, Chief Medical Officer at PuRxCell and at PUR-FORM, Professor of Regenerative Medicine at UniMax University in Indatuba Brazi, shared a post on LinkedIn:
“Immune Privilege versus Immune Evasion: Why MSCs Are Not What We Thought
When I was lecturing recently, I included a few slides on immune privilege and immune evasion in cells.
I wrote this article to clarify the difference between immune privilege and immune evasion, using MSCs and MUSE cells to illustrate why this distinction matters for allogeneic cell therapy.
Immune privilege is a state in which immune ‘guards’ are physically and chemically kept out of certain body sites (such as the eye or placenta), allowing foreign cells to survive indefinitely without mounting an immune response or relying on drugs.
Immune evasion, by contrast, means the immune system does encounter the transplanted cells, but those cells actively secrete calming signals that suppress or distract immune attack.
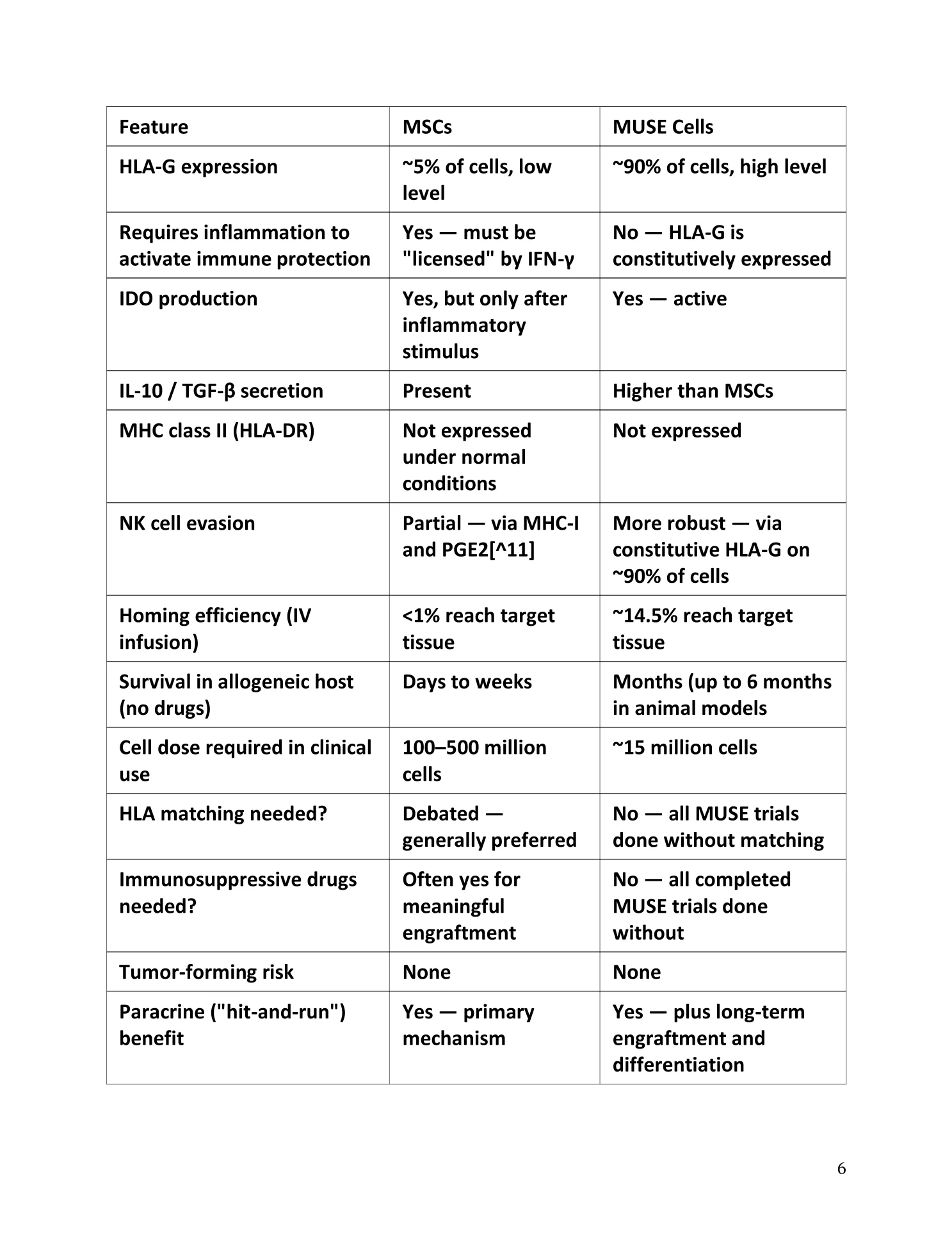
This strategy is conditional and can eventually fail. MSCs are presented as potent but conditionally immune-evasive cells: they upregulate their immunosuppressive machinery only when exposed to inflammatory cues such as interferon-gamma, at which point they deploy tools like IDO (tryptophan depletion and kynurenine production), PGE2, TGF-β, IL-10, and limited HLA-G expression to dampen T cells, NK cells, and pro-inflammatory macrophages.
Because this response is reactive and depends on ongoing inflammatory signaling, MSCs are no longer considered truly immune – privileged; instead, they may be rejected once their evasive signaling wanes, limiting their durability as universal ‘off-the-shelf’ therapies compared with genuinely immune – privileged cells such as MUSE cells. JP”
Rowan Paul, Sports Medicine and Interventional Regenerative Orthobiologics Physician at RegenCore, shared this post on LinkedIn:
“Immune privilege versus Immune evasive.
There are key differences that affect the way we think about allogeneic cellular therapies. MUSE cells are immune privileged.
Traditional allogeneic MSC are Immunoevasive.
This may affect the biological kinetics of the paracrine effect, the ability and timeliness of engraftment, and in particular safety profile based on immunity reactivity.
Autologous MSC of course don’t have to hide which is a key benefit but have their own benefits and limitations and risk due to harvesting, dosing age, and functionality over time.”
 Stay updated with Hemostasis Today.
Stay updated with Hemostasis Today.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-
Jun 23, 2026, 18:27Advancing Gene Therapy Research for Glanzmann Thrombasthenia – Glanzmann’s Research Foundation
-
Jun 23, 2026, 18:17What Every ITP Patient Wants to Know – ITP Support Association
-
Jun 23, 2026, 18:13Ahsan Fareed: Exploring Heart Failure Readmissions in Iron Deficiency Anemia
-
Jun 23, 2026, 18:09Swarnava Roy: Key Findings on Stress Erythropoiesis and Mitochondrial Retention in RBCs
-
Jun 23, 2026, 17:40Hossam El Benawi: How do We Predict Recurrence Post LVT Resoultion?
-
Jun 23, 2026, 17:39Nicolas Gendron: Do We Really Need All These Hemostasis Tests in Patients on DOACs?
-
Jun 23, 2026, 17:33Maité Mulkers: Time is Brain, and One Reason is That a Thrombus Develops Over Time
-
Jun 23, 2026, 17:32Dhargam Aljebouri: Honoured to Be Part of the Young Professionals Breakfast at ISBT 2026
-
Jun 23, 2026, 17:27Dianne E. van der Wal: Phenotype and Activation of the Endothelium in ET at ISTH 2026