
Tasawar Siddique: Early Detection of Nephrotic Syndrome
Tasawar Siddique, Surgery Resident, Graduate Student at The Third Xiangya Hospital Of Central South University, shared a post on LinkedIn:
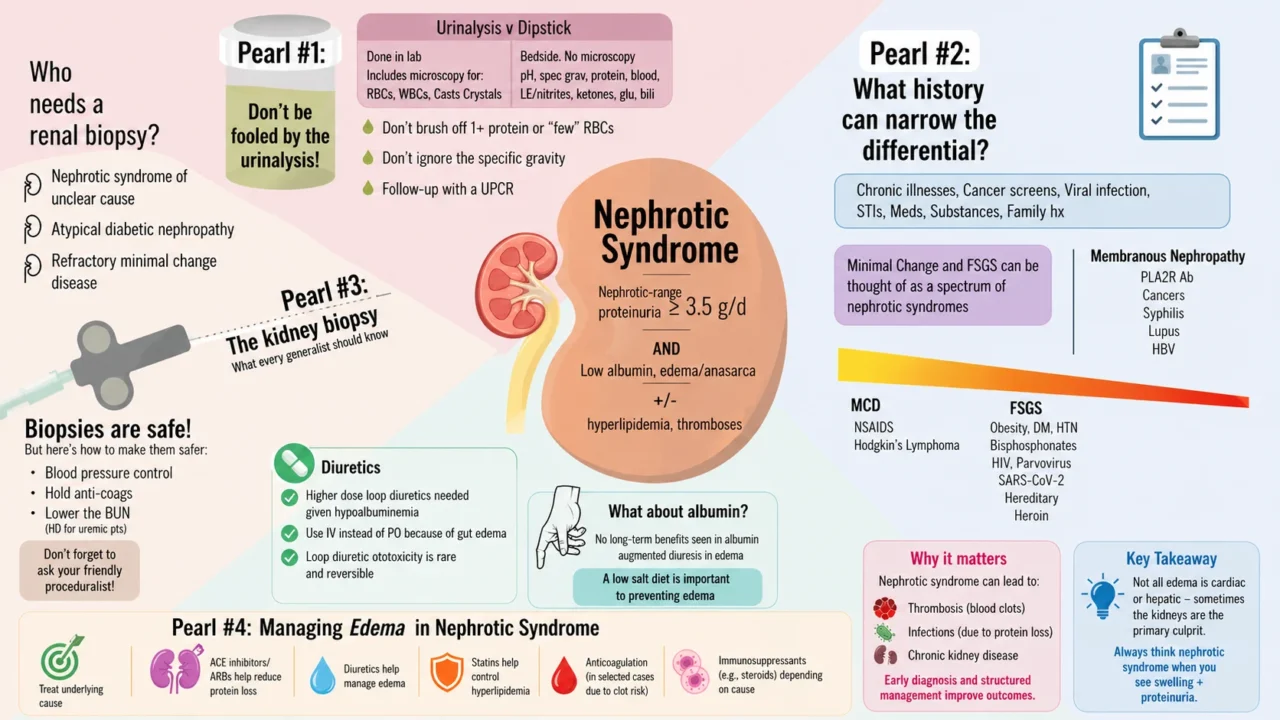
”Nephrotic Syndrome – What Every Clinician Should Recognize Early
Nephrotic syndrome is more than just ‘protein in urine.’
It’s a glomerular (kidney filter) disorder that leads to significant protein loss, fluid imbalance, and increased risk of complications. Early recognition can prevent long-term kidney damage and systemic effects.
What is Nephrotic Syndrome?
In simple terms, the kidneys start ‘leaking protein.’
Medically, it’s defined by:
- Heavy proteinuria (greater than 3.5 g/day)
- Hypoalbuminemia (low blood protein)
- Edema (swelling)
- Hyperlipidemia
Common Causes
- Primary (kidney-related): Minimal change disease, FSGS, membranous nephropathy
- Secondary: Diabetes mellitus, lupus, infections, drugs
Clinical Features (What You’ll See)
- Generalized swelling (face, legs, abdomen)
- Frothy or ‘bubbly’ urine
- Weight gain due to fluid retention
- Fatigue, reduced urine output in some cases
Key Investigations
- Urine analysis shows proteinuria
- Serum albumin is low
- Lipid profile shows elevated cholesterol
- Renal function tests
- Kidney biopsy (when indicated)
Management Principles
- Treat underlying cause
- ACE inhibitors/ARBs help reduce protein loss
- Diuretics help manage edema
- Statins help control hyperlipidemia
- Anticoagulation (in selected cases due to clot risk)
- Immunosuppressants (e.g., steroids) depending on cause
Why It Matters
Nephrotic syndrome can lead to:
- Thrombosis (blood clots)
- Infections (due to protein loss)
- Chronic kidney disease
Early diagnosis and structured management improve outcomes significantly.
Clinical Insight
From hospital wards to remote telehealth settings, understanding nephrotic syndrome helps clinicians guide patients, monitor labs, and manage complications effectively – even at a distance.
Takeaway
Not all edema is cardiac or hepatic – sometimes the kidneys are the primary culprit.
Always think nephrotic syndrome when you see swelling and proteinuria.”
Stay updated with Hemostasis Today.
-
Aug 11, 2026, 08:20Hasan Abbas Zaheer: Strengthening Universal Access to Safe Blood in Pakistan
-
Aug 11, 2026, 08:07Nicola Pozzi: Advancing Hemostasis Through Scientific Collaboration at Hemostasis GRC
-
Aug 11, 2026, 07:50When Access to Care Changes Everything – WFH
-
Aug 11, 2026, 07:41Kevin Land: How Cellular Therapy Is Changing Transfusion Medicine
-
Aug 11, 2026, 07:35Kuldeep Singh Bhadauria: Building the Future of Hemophilia Care in India
-
Aug 11, 2026, 07:28Archil Jaliashvili: When Every Minute Matters Time Becomes a Therapy
-
Aug 11, 2026, 07:05Mavis Agnes Kisakye: Building Sustainable Transition Pathways in Hemophilia Care
-
Aug 11, 2026, 06:48Rishdha Roshad: What Happens to the Brain During Cardiopulmonary Bypass?
-
Aug 11, 2026, 05:53Isaac Okello: Strengthening Sickle Cell Advocacy in Uganda