

Heghine Khachatryan: Heavy Menstrual Bleeding in Women with Bleeding Disorders – Key Insights from WFH 2026
Heghine Khachatryan, Editor-in-Chief of Hemostasis Today and Head of the Hemophilia and Thrombosis Center at the Yeolyan Hematology and Oncology Center, shared posts on LinkedIn about key insights from Day 2 of the World Federation of Hemophilia (WFH) 2026 Congress:
“WFH 2026 | Day 2
Heavy Menstrual Bleeding: The Most Underrecognized Gateway to Bleeding Disorders
One of the most clinically important and practice-changing sessions today focused on Heavy Menstrual Bleeding (HMB) – not merely as a gynecological complaint, but as a key diagnostic window into underlying bleeding disorders.
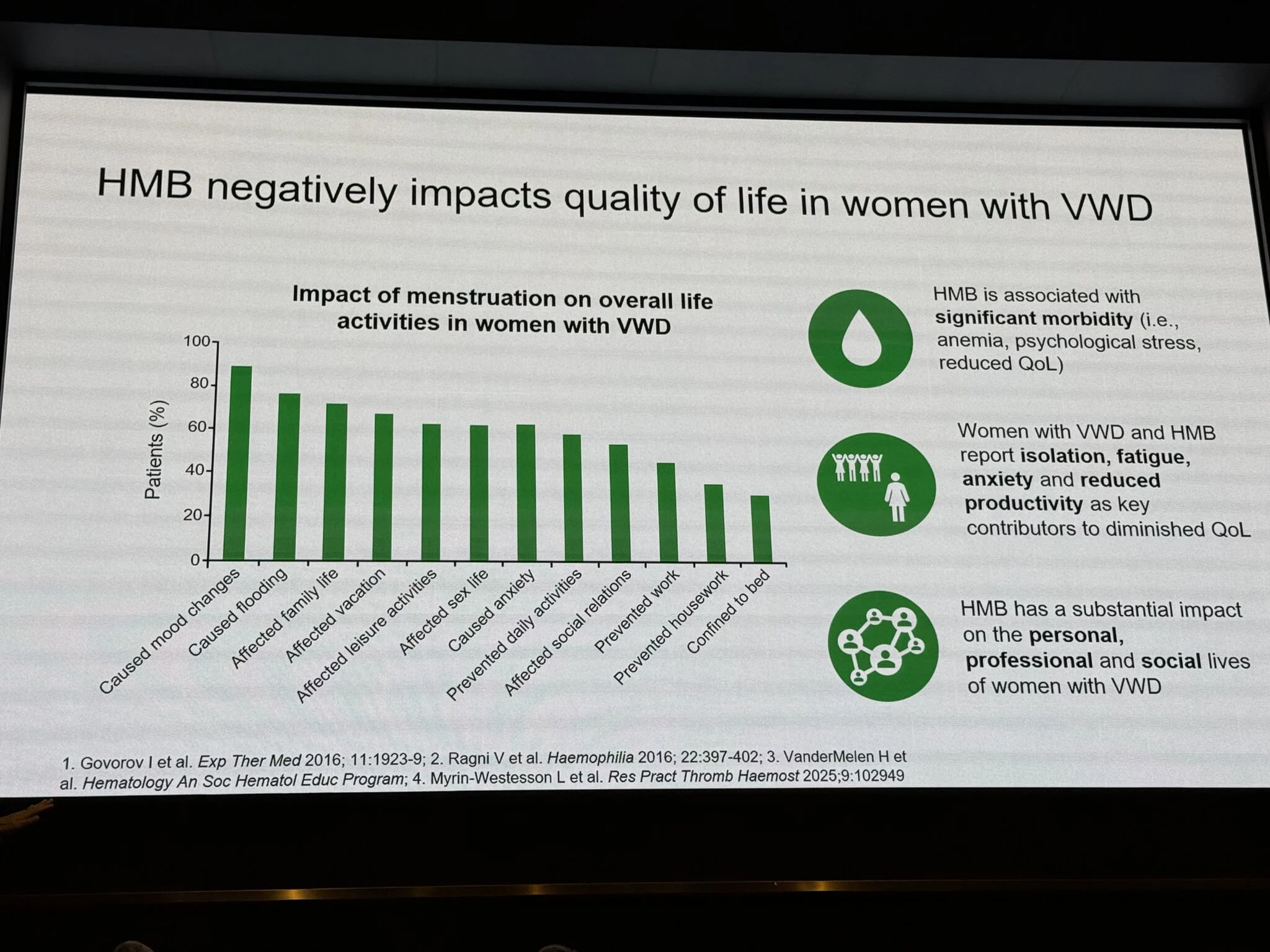
Reframing HMB: from symptom to signal
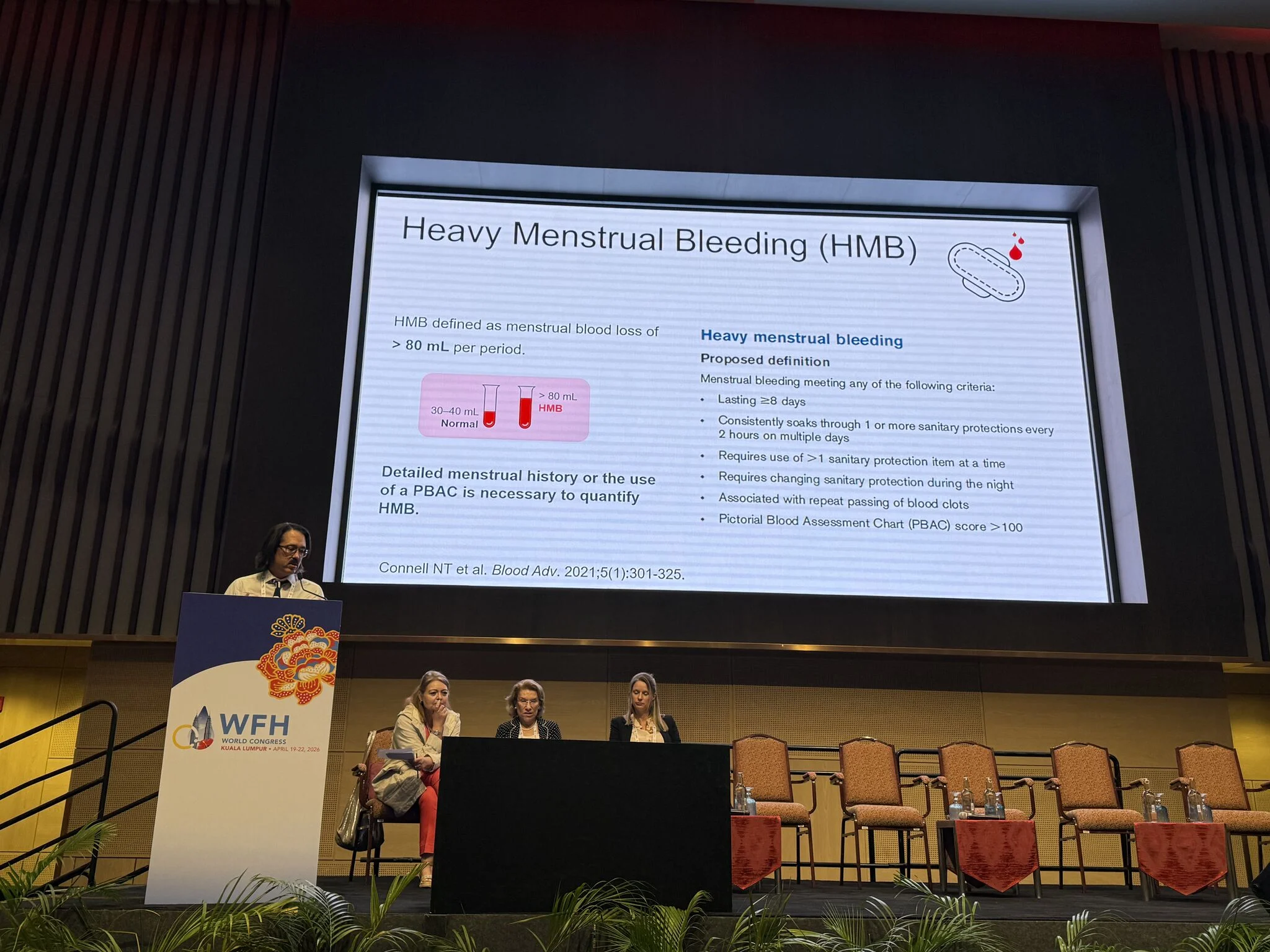
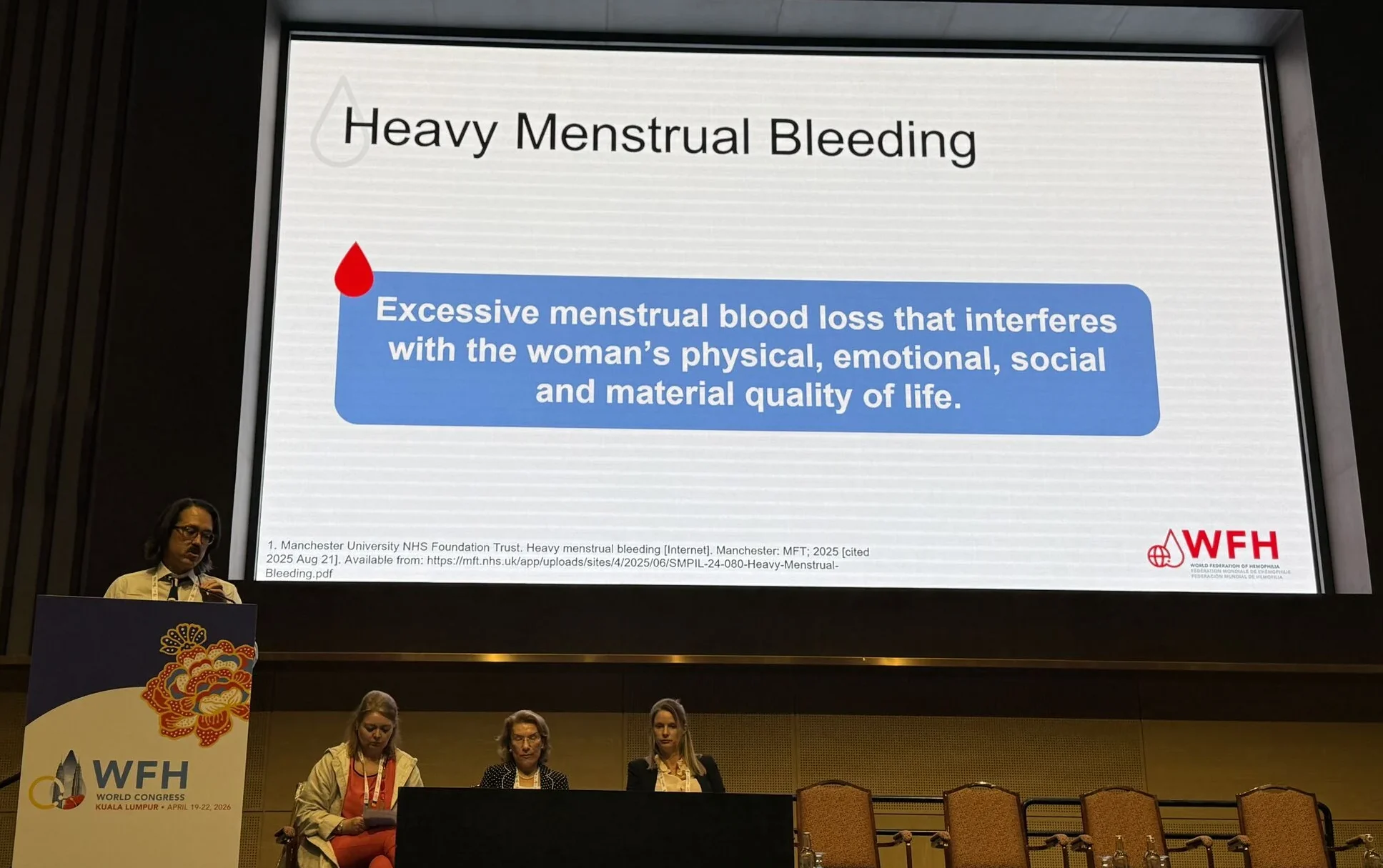
HMB is defined not only quantitatively (>80 mL per cycle), but more importantly by its impact on quality of life:
- Physical
- Emotional
- Social
- Economic
This functional definition is critical, especially in settings where objective measurement is limited.
The hidden epidemiology
A striking message:
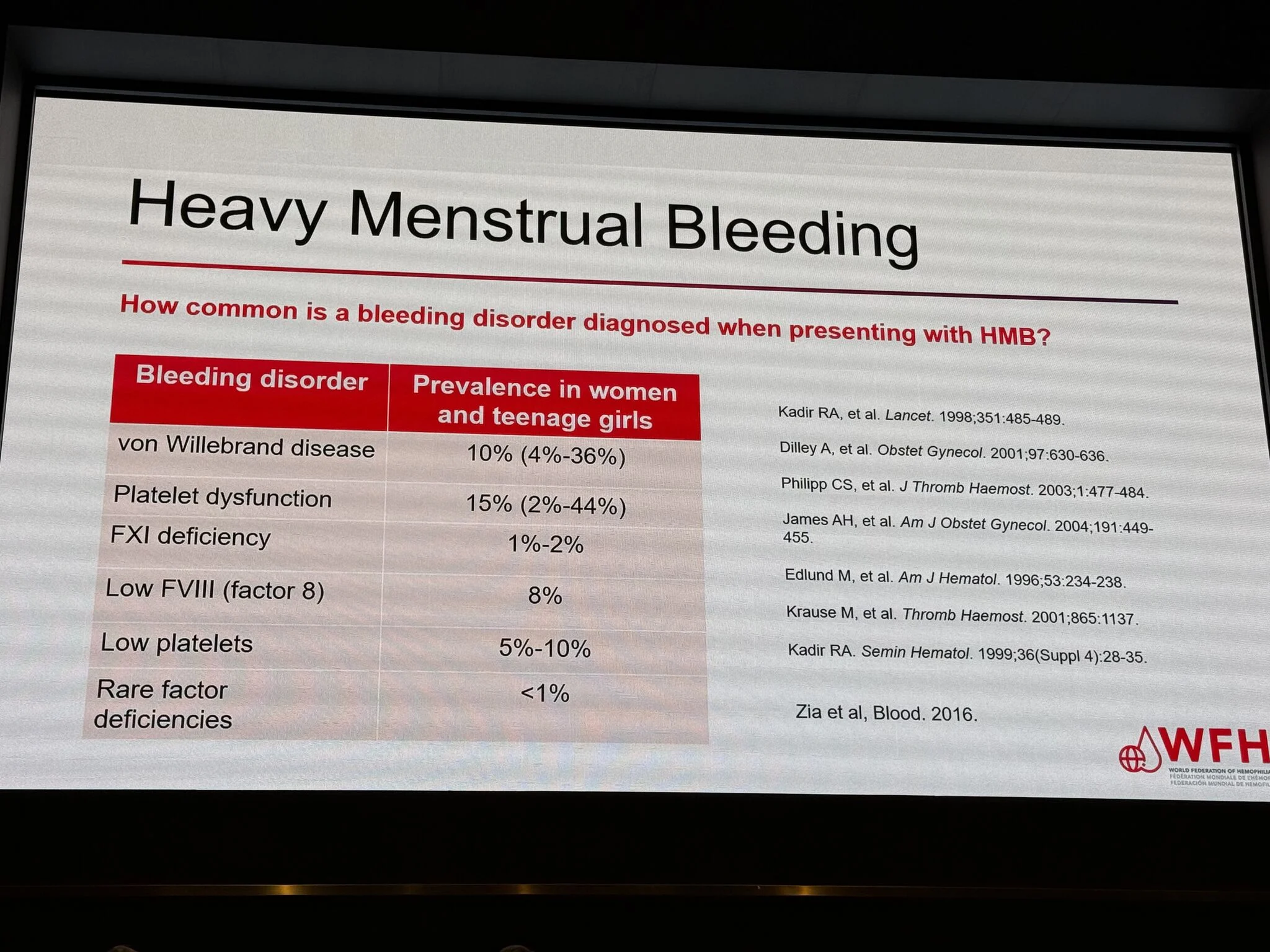
A substantial proportion of women presenting with HMB have an underlying hemostatic disorder.
Key data:
- von Willebrand disease leads to ~10%
- platelet dysfunction leads to ~15%
- factor deficiencies (including FVIII) lead to a significant subset
- thrombocytopenia leads to up to 10%
Yet, the majority remain undiagnosed or diagnosed late
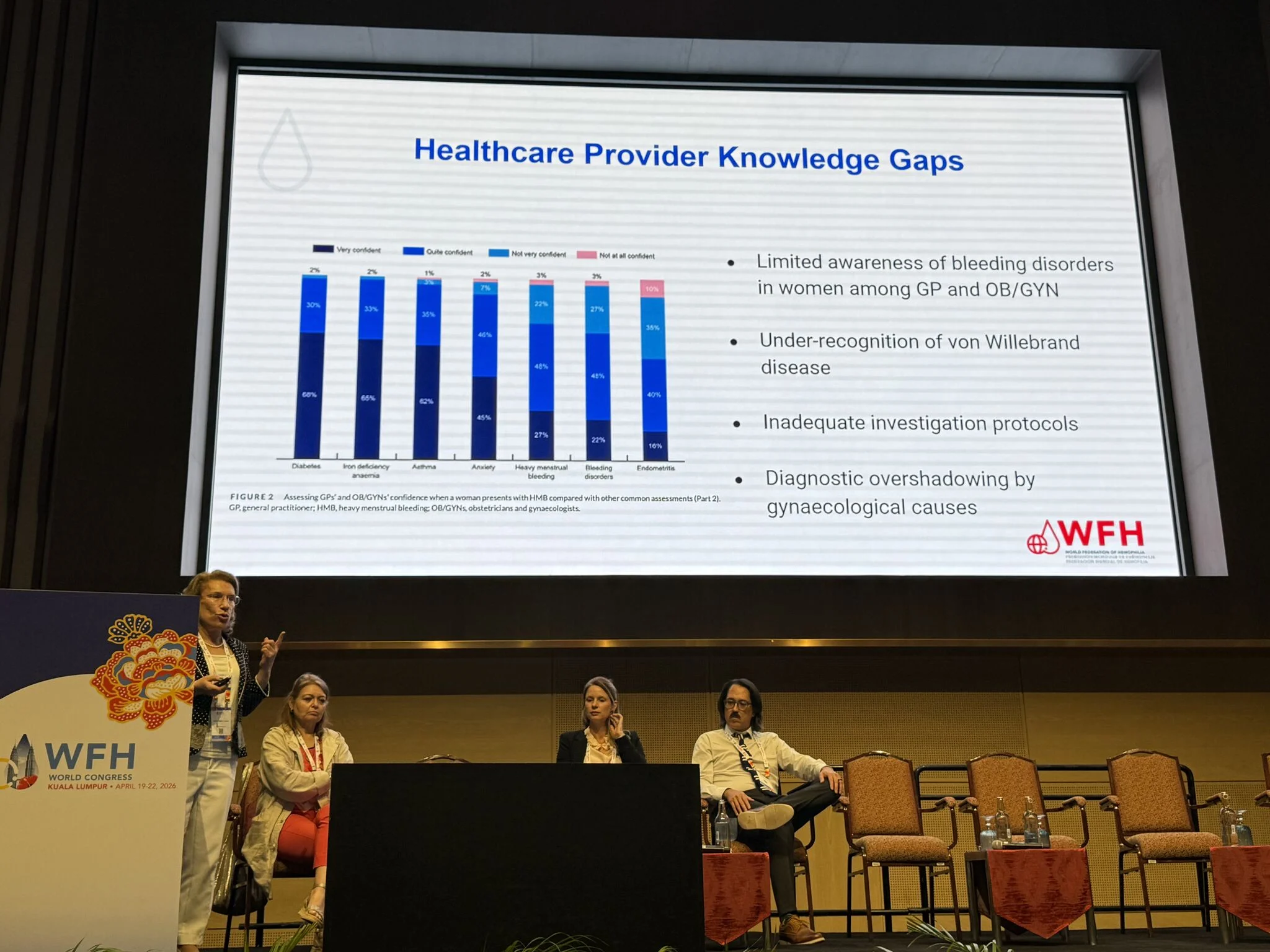
Diagnostic gap: where we fail
Despite available guidelines, identification remains inconsistent.
Challenges include:
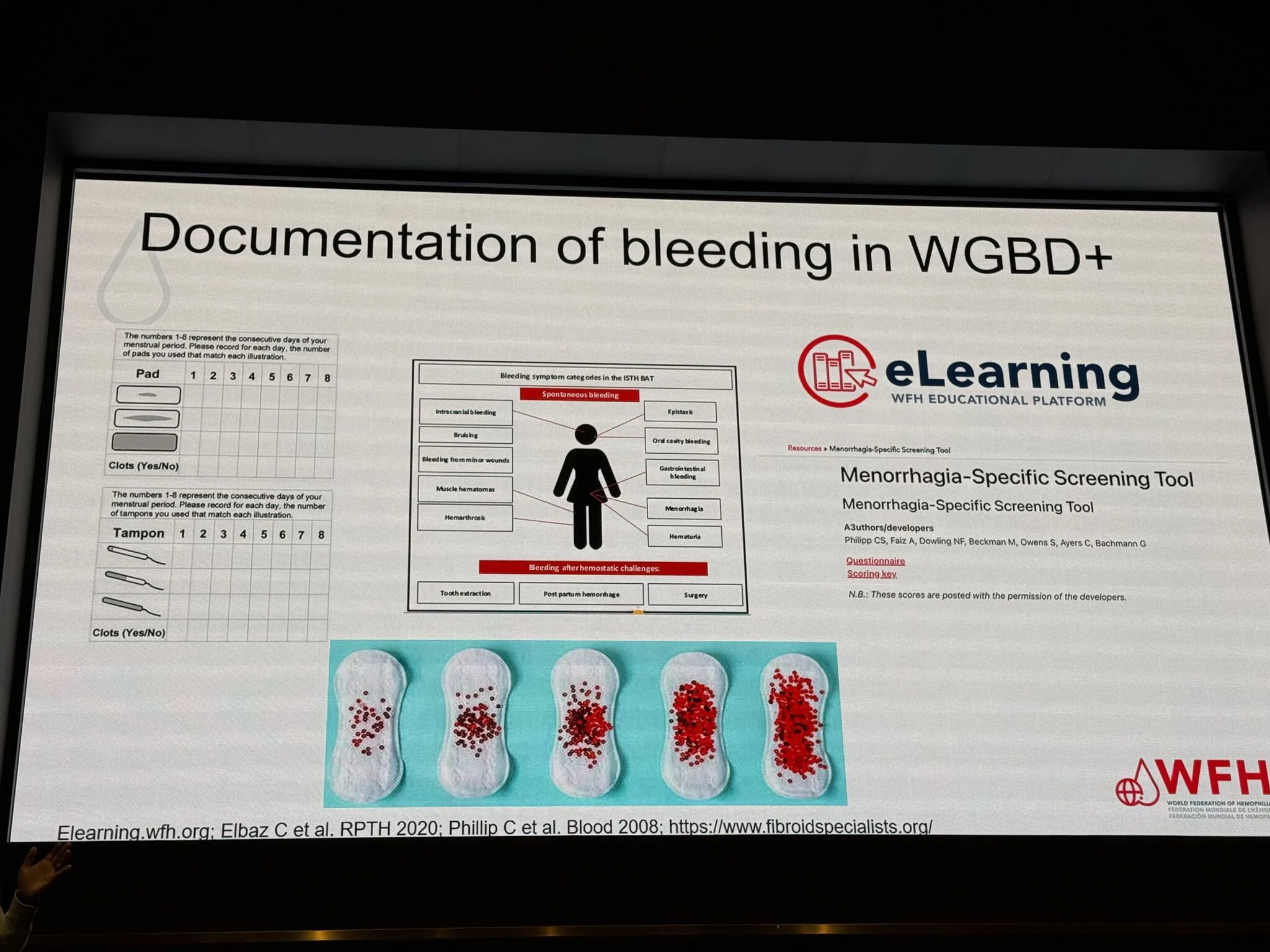
- Lack of structured bleeding history
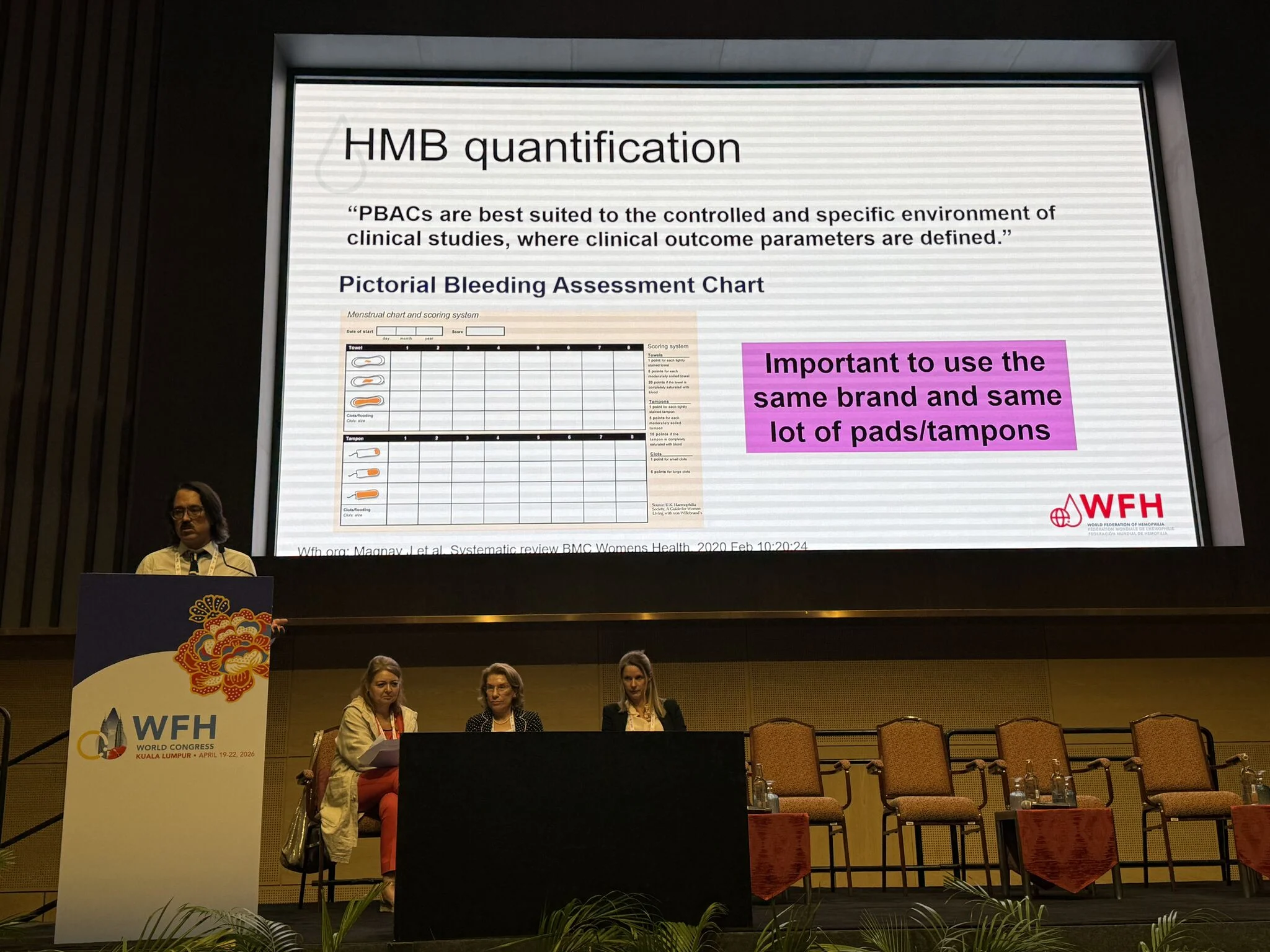
- Underutilization of standardized tools (ISTH-BAT, PBAC)
- Limited integration between hematology and gynecology
- Variable clinician awareness
‘HMB is often treated – but not investigated’
What should we do better?
The session strongly emphasized a systematic approach:
Clinical assessment
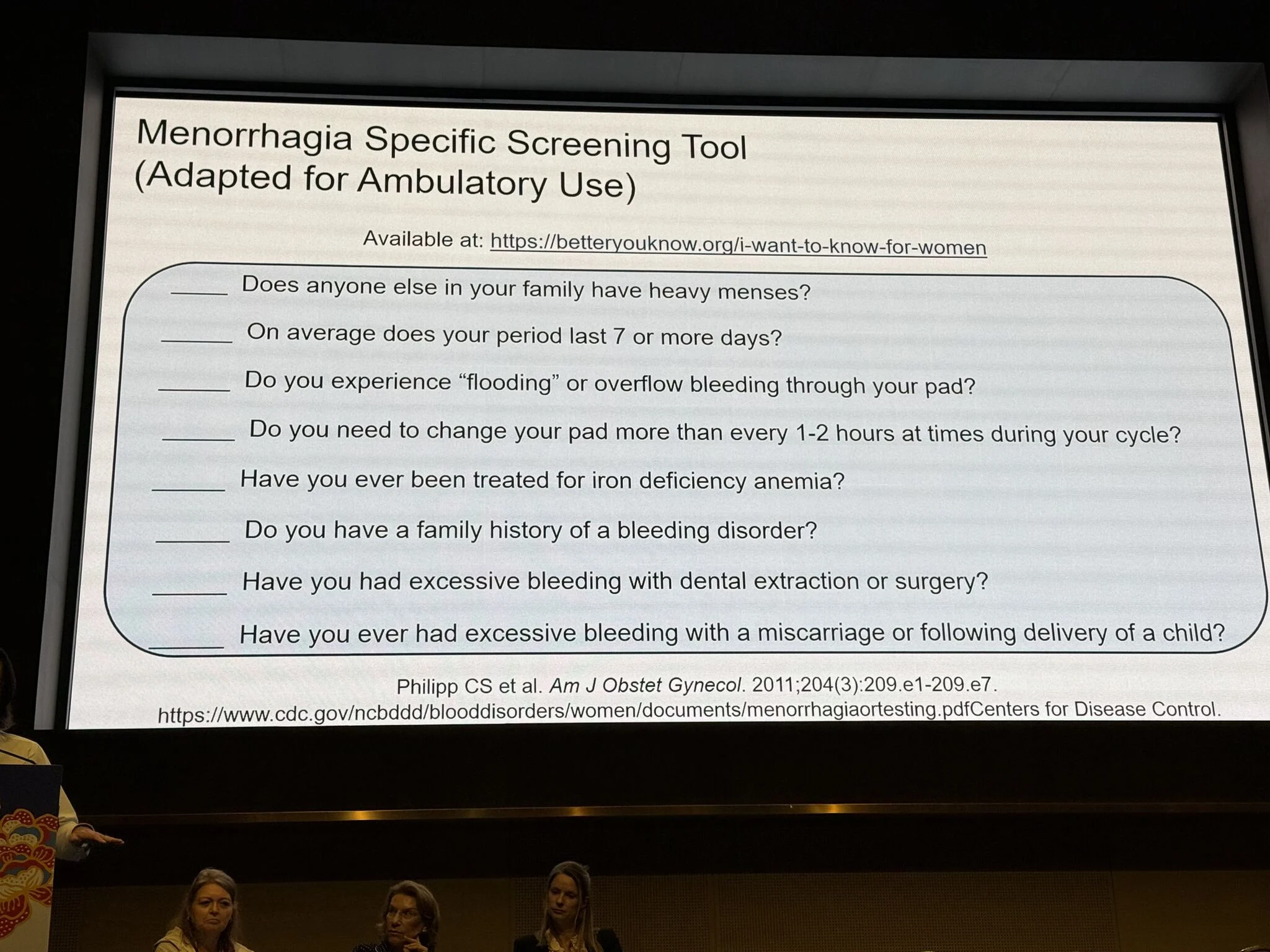
- Detailed menstrual history
- Use of PBAC scoring
- Screening for bleeding symptoms across systems
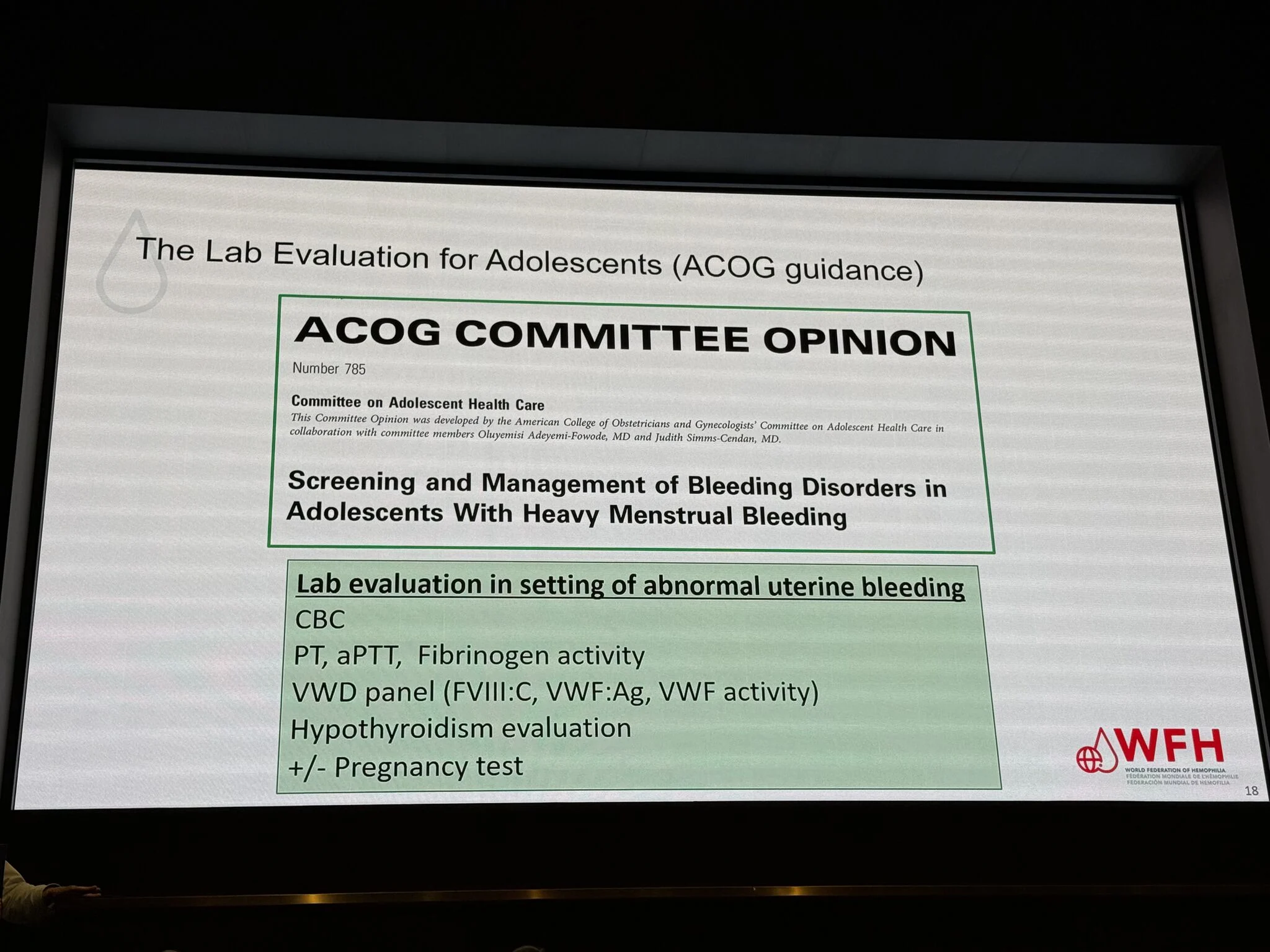
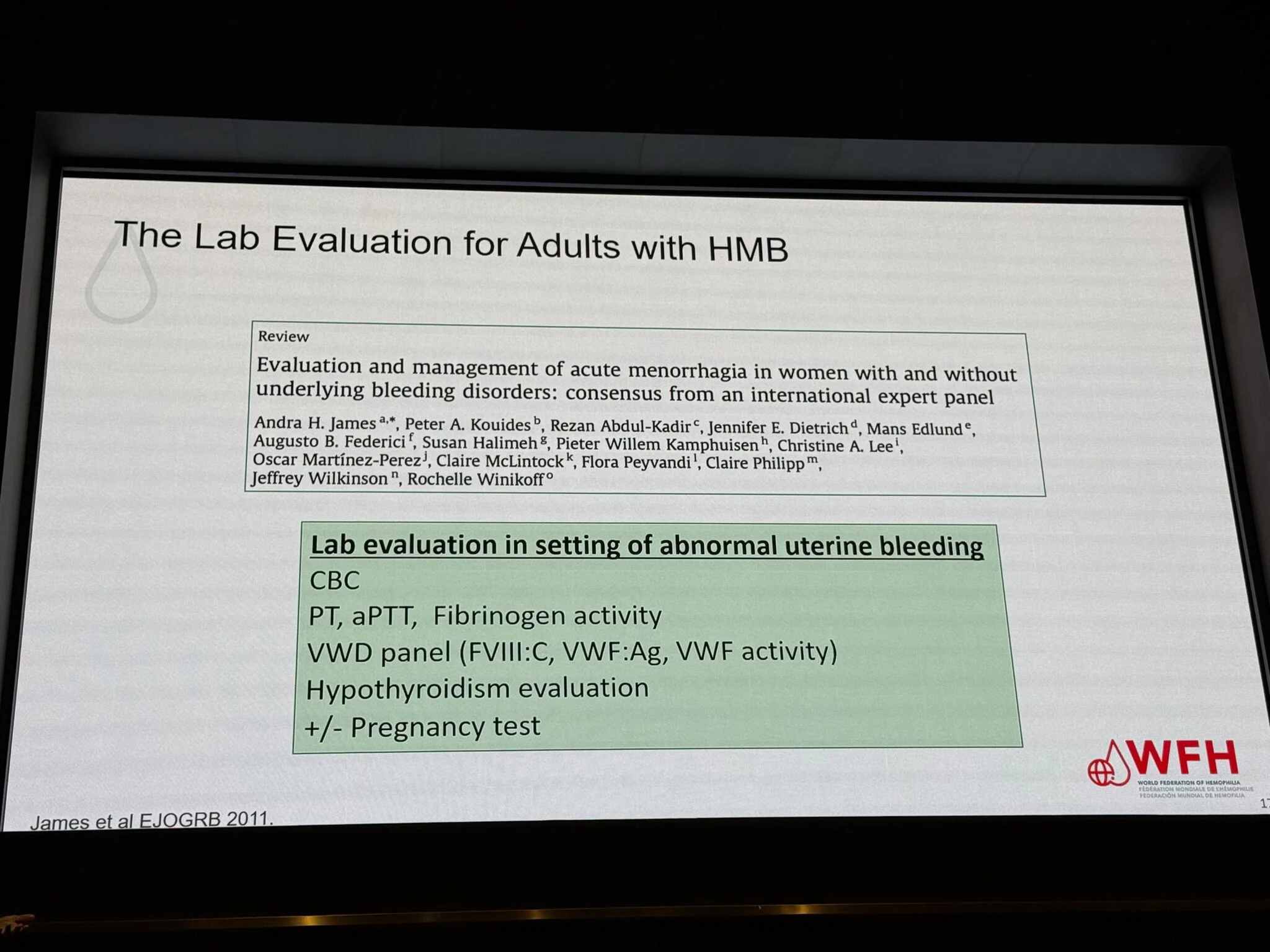
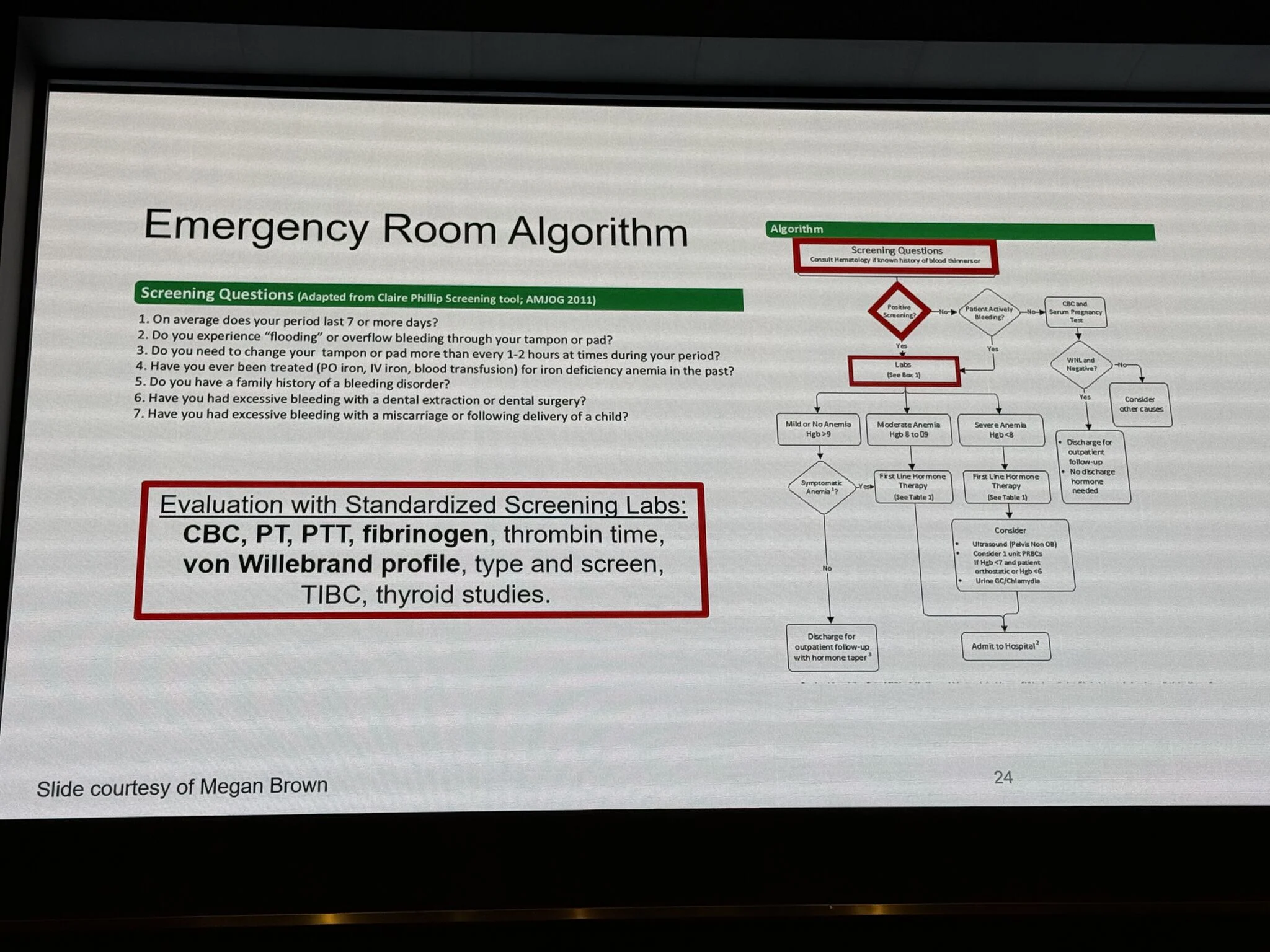
Laboratory evaluation (aligned with ACOG / international guidance)
- CBC
- PT, aPTT, fibrinogen
- VWD panel (FVIII:C, VWF:Ag, VWF activity)
- Thyroid function
- with or without pregnancy testing
Adolescents: a critical window
HMB in adolescence is particularly important:
Often the first clinical manifestation of a bleeding disorder
Early diagnosis can prevent:
- chronic anemia
- unnecessary gynecologic interventions
- long-term morbidity
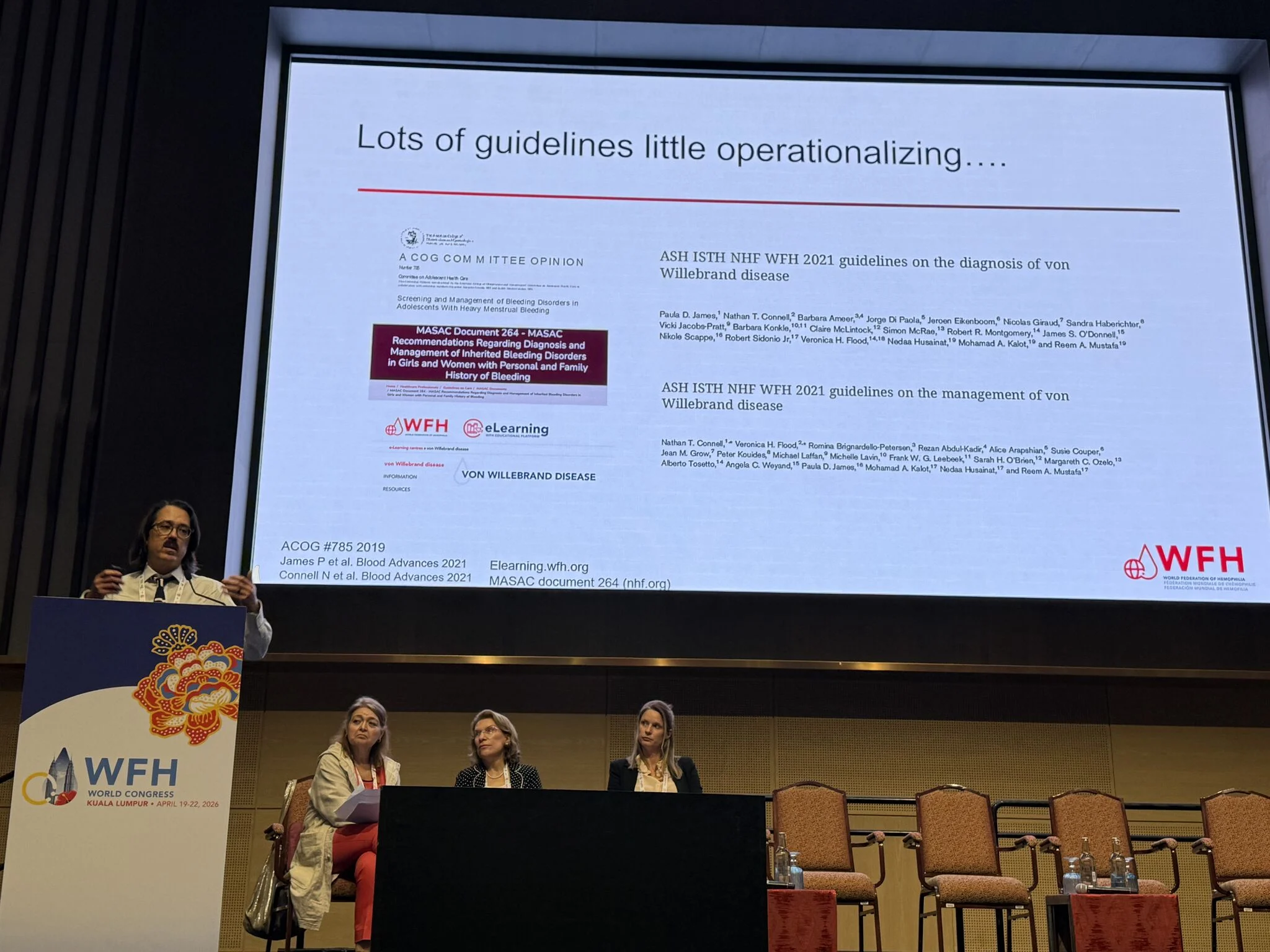
From guidelines to implementation
A key critical insight:
We have guidelines – but limited operationalization
Multiple high-level recommendations exist (ACOG, ASH/ISTH/WFH), yet:
- Screening pathways are not standardized
- Tools are not routinely used in practice
- Multidisciplinary care remains fragmented
Strategic takeaway
Heavy menstrual bleeding is not just a symptom – it is a diagnostic opportunity we are still missing globally.
Closing this gap requires:
- integration of hematology into women’s health
- structured screening pathways
- education of frontline clinicians
- accessible diagnostic infrastructure
If we identify HMB correctly, we identify bleeding disorders earlier.
If we miss it – we miss the patient.”

See more in the gallery.
“WFH 2026 | Heavy Menstrual Bleeding in Women with Bleeding Disorders
This session distilled a key message: heavy menstrual bleeding (HMB) is a hemostatic disorder requiring structured, risk-adapted management.
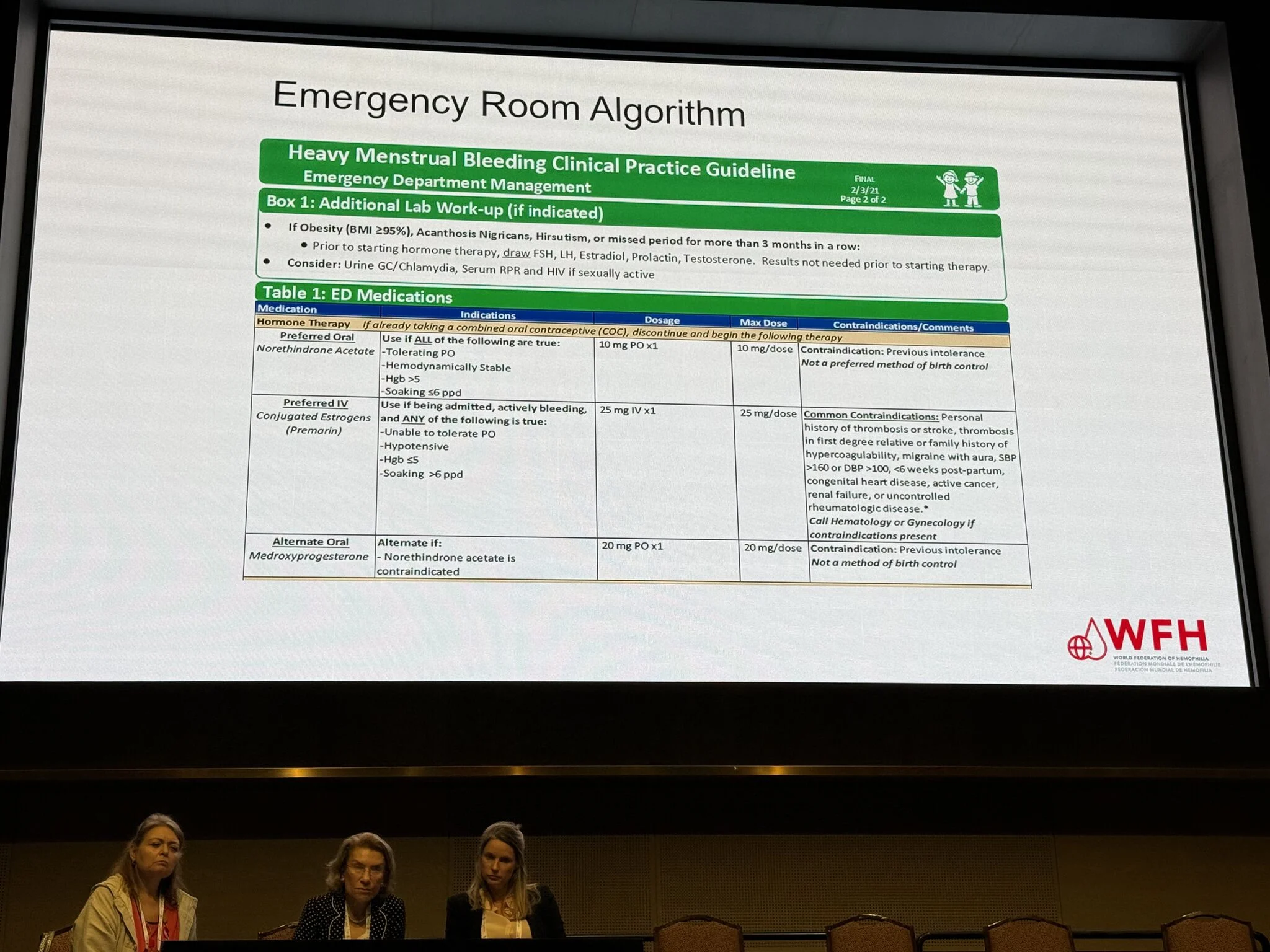
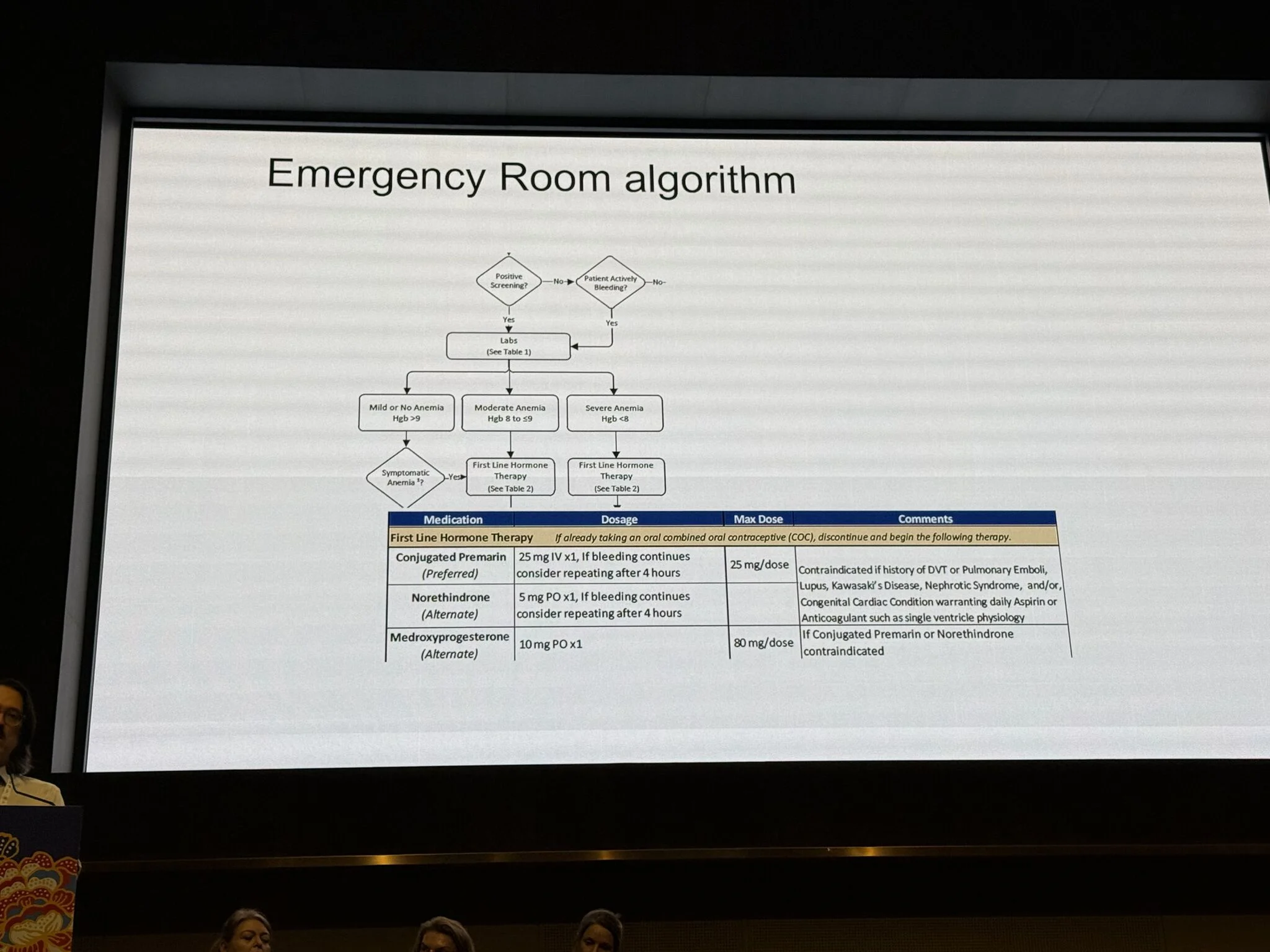
Acute management (algorithm-based)
- First line: COCs or high-dose estrogen
- If contraindicated: progestin-only regimens
- If persistent bleeding: add antifibrinolytics with or without tamponade; involve hematology
Critical nuance: Estrogen is contraindicated in patients with thrombotic risk (e.g., prior VTE, migraine with aura, hypertension), thus requiring individualized therapy.
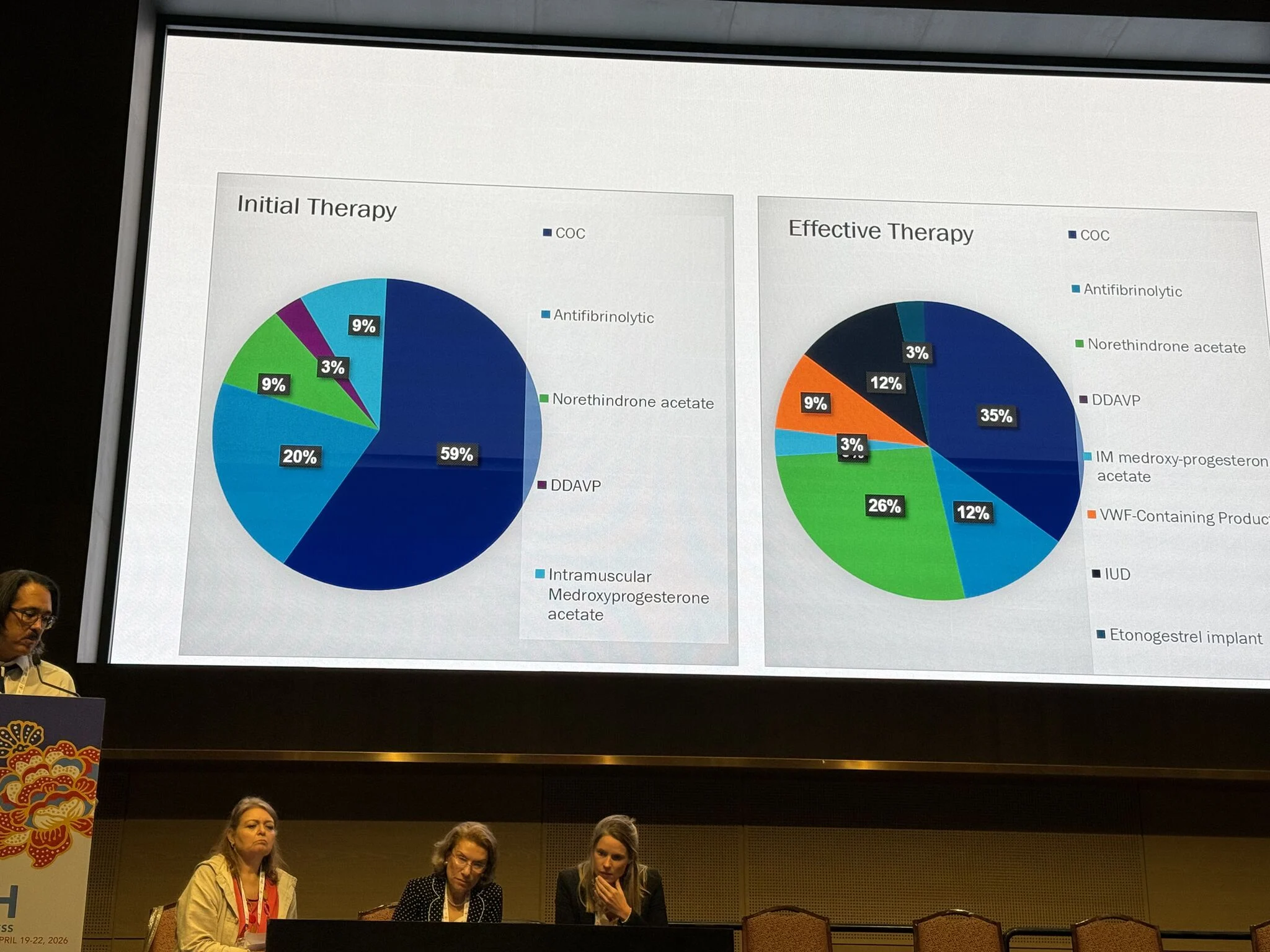
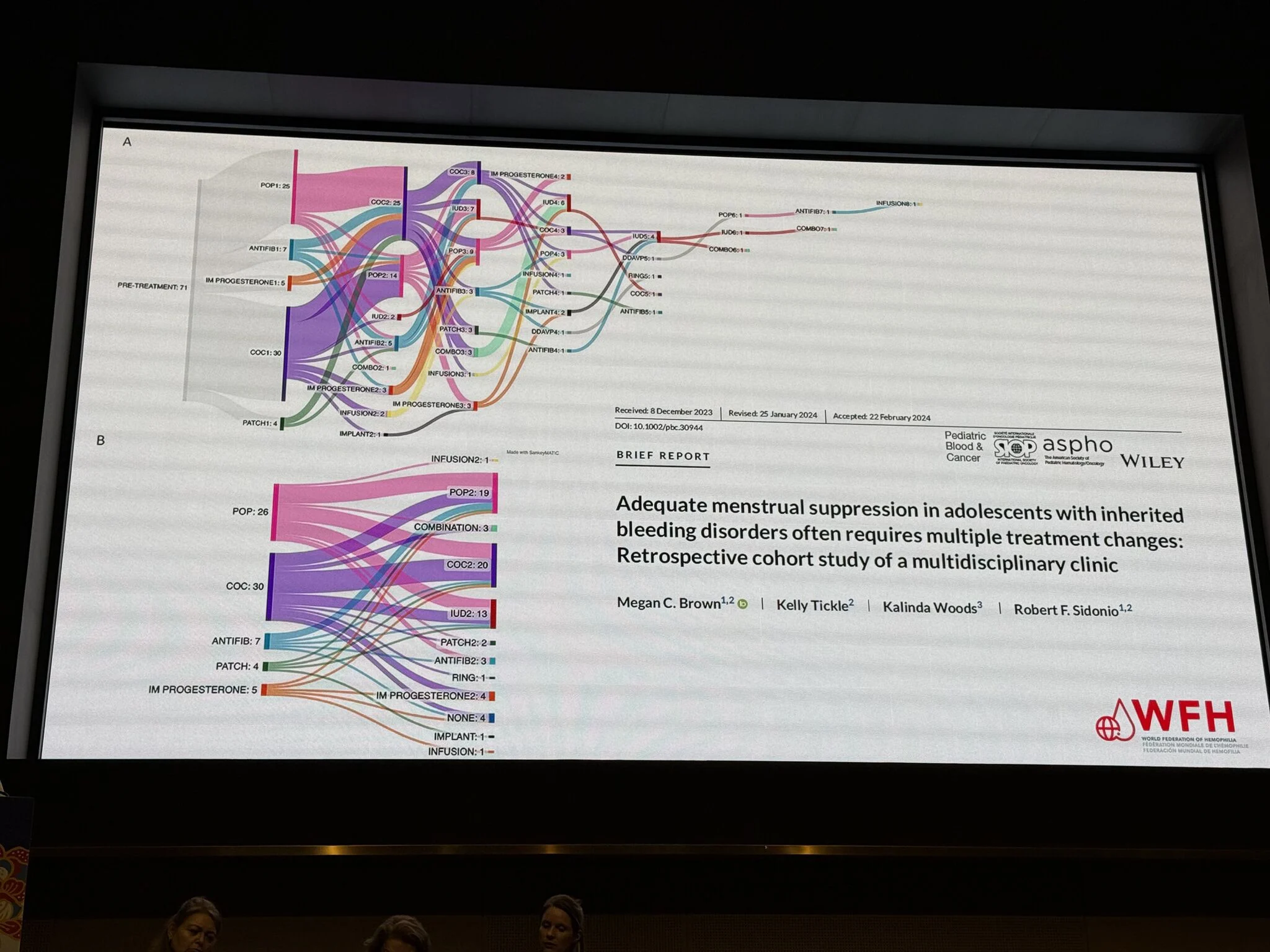
From initiation to effective therapy
- Initial approach: predominantly COCs (~59%)
- Effective control: shift toward multimodal strategies
- Progestins
- Antifibrinolytics
- DDAVP / VWF-containing therapies
- LARC (IUD, implant)
Single-modality therapy is often insufficient
Treatment dynamics
Frequent switching (COC to progestin to antifibrinolytic to device/combination) reflects:
Expected therapeutic adaptation, not failure
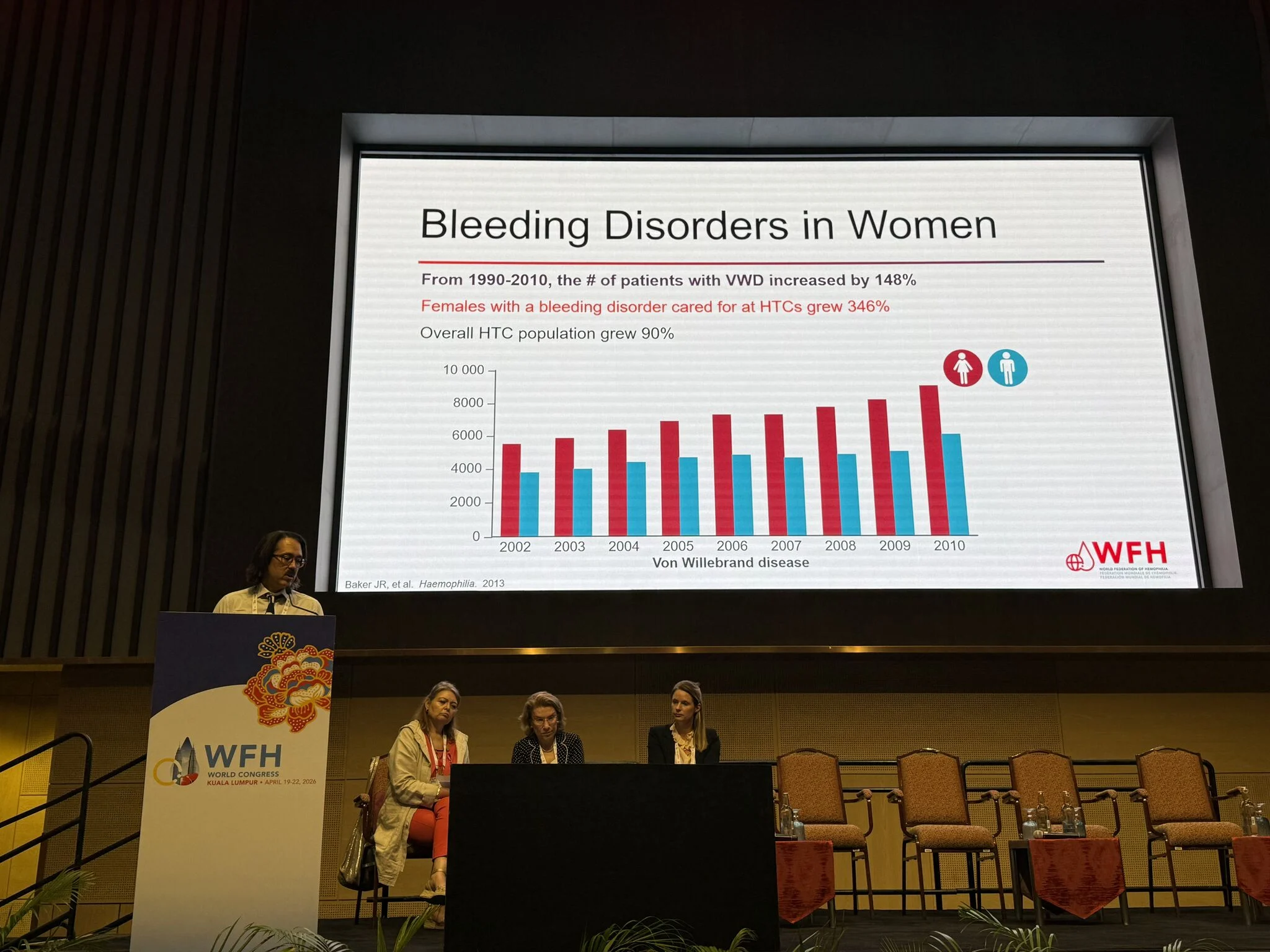
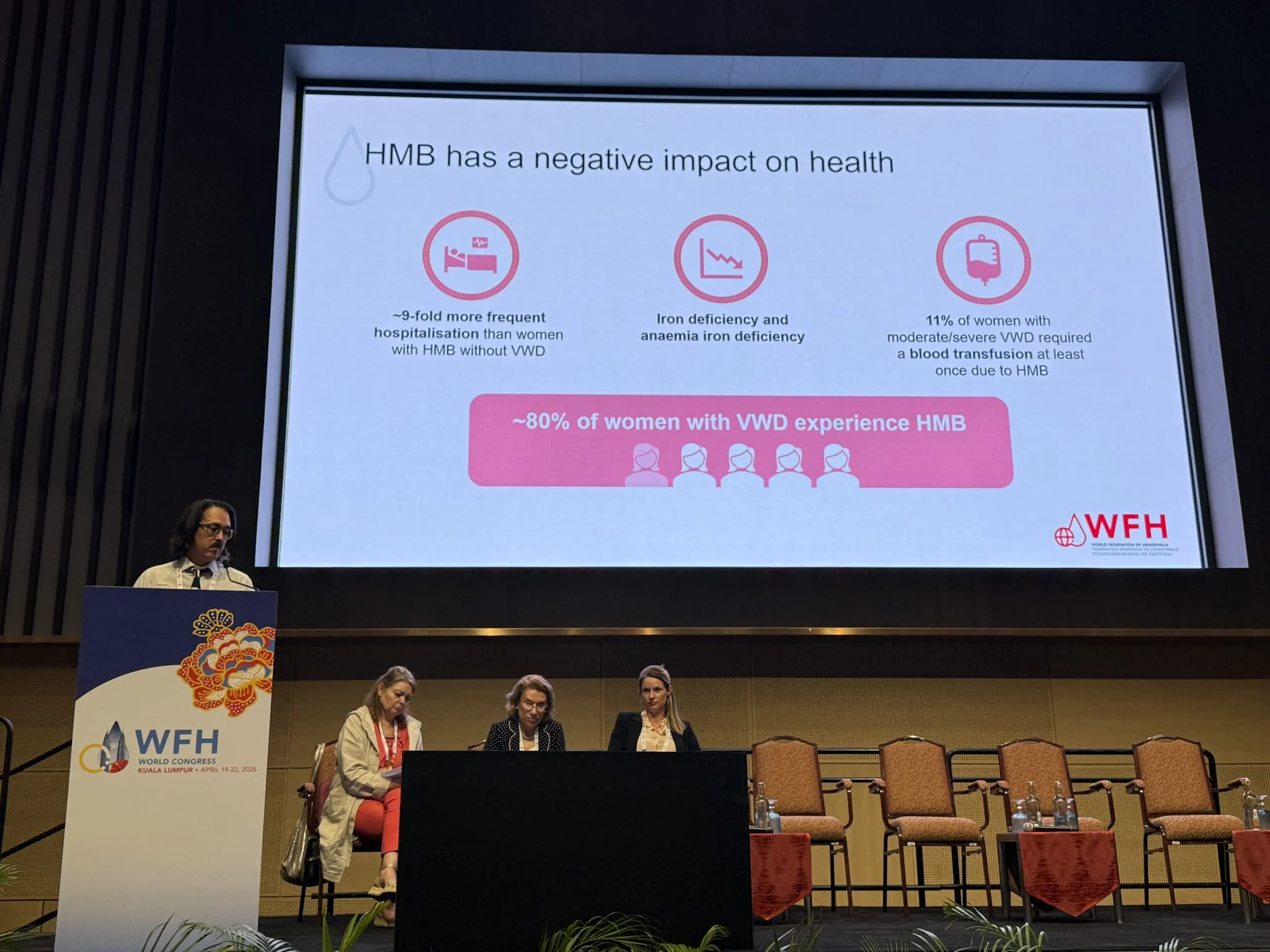
Epidemiology and delay
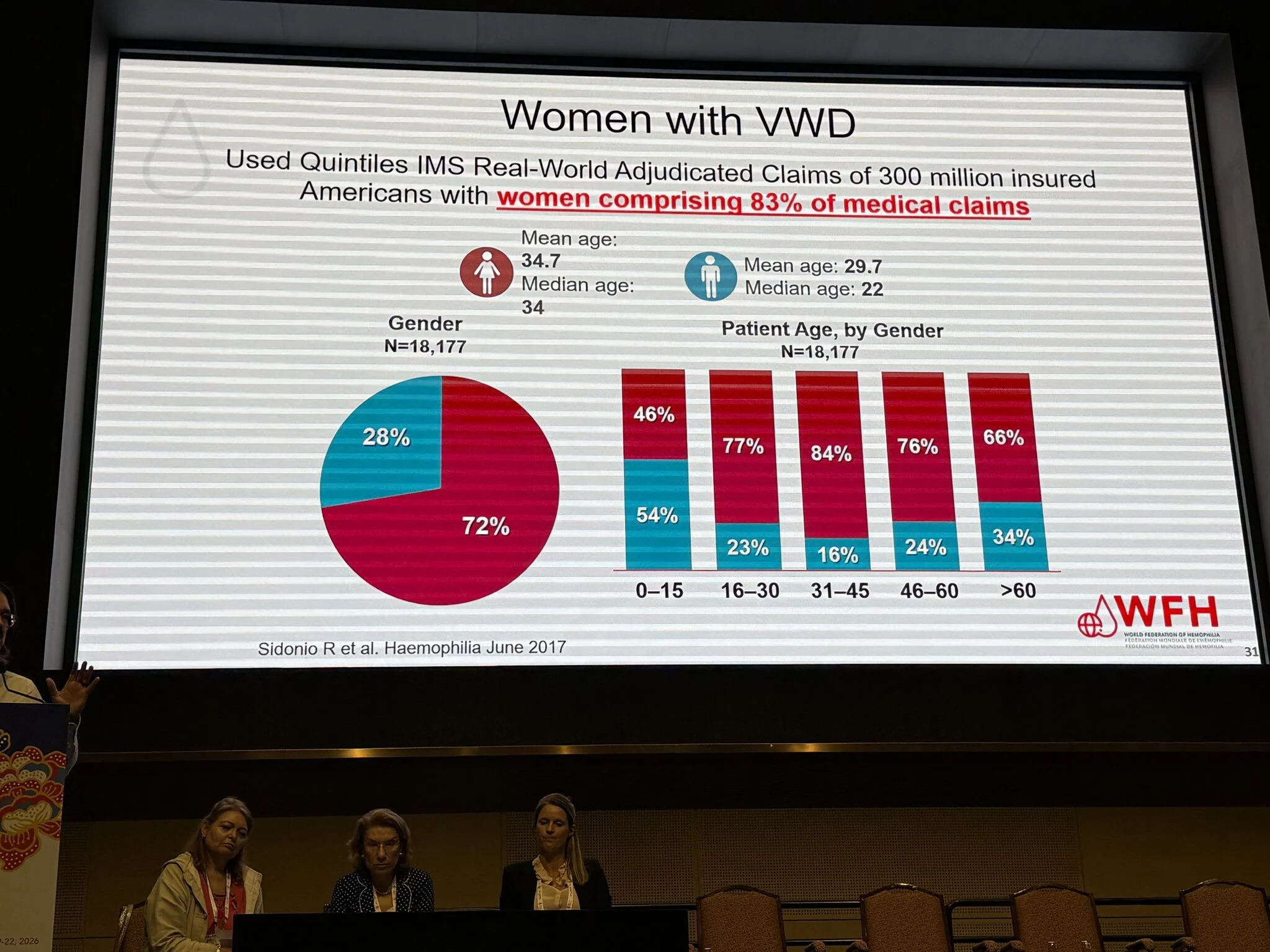
- Women represent ~72% of VWD cases
- Account for ~83% of claims
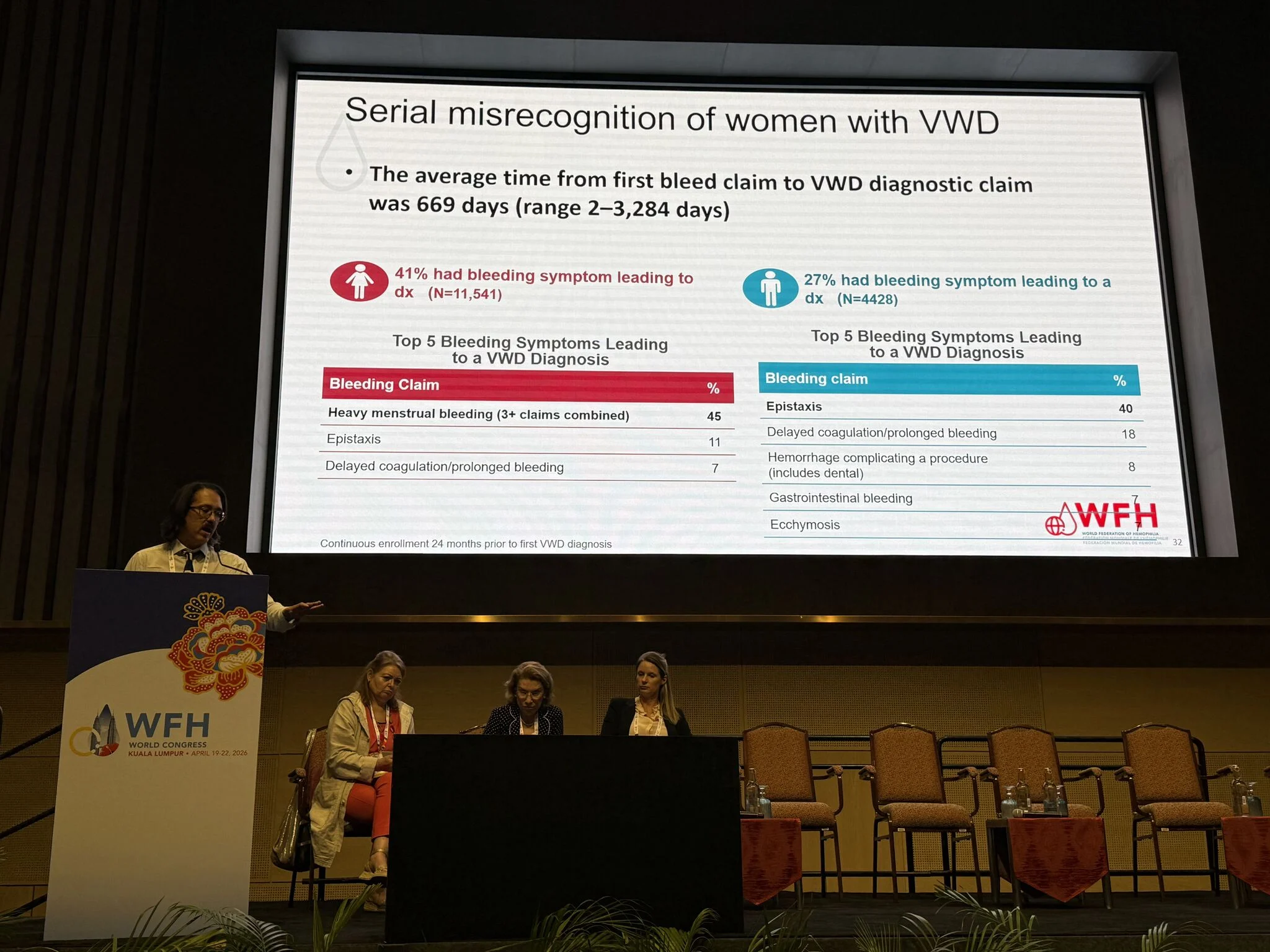
- Diagnostic delay ≈ 669 days
Leads to anemia, reduced QoL, and late specialist referral.
Core problem: misrecognition
- Women: HMB (≈45%) drives diagnosis
- Men: epistaxis predominates
Menstrual bleeding remains under-recognized as a pathological signal
Clinical takeaway
HMB should be approached as a hematologic condition until proven otherwise
What must change
- Routine HMB screening
- Earlier hematology referral
- Gynecology–hematology integration
- Risk-adapted therapy (bleeding vs thrombosis balance).”

See more in the gallery.
“Beyond Biology: Menstrual Stigma as a Systemic Barrier in Hemostasis Care
At the World Federation of Hemophilia Congress 2026, Rezan Abdul Kadir delivered a compelling and methodologically grounded analysis of an often-overlooked determinant of diagnostic delay in women with bleeding disorders: menstrual stigma as a structural phenomenon.
This session moved decisively beyond descriptive narratives, framing menstruation within multi-level socio-medical constructs that directly influence clinical outcomes.
Key analytical insights:
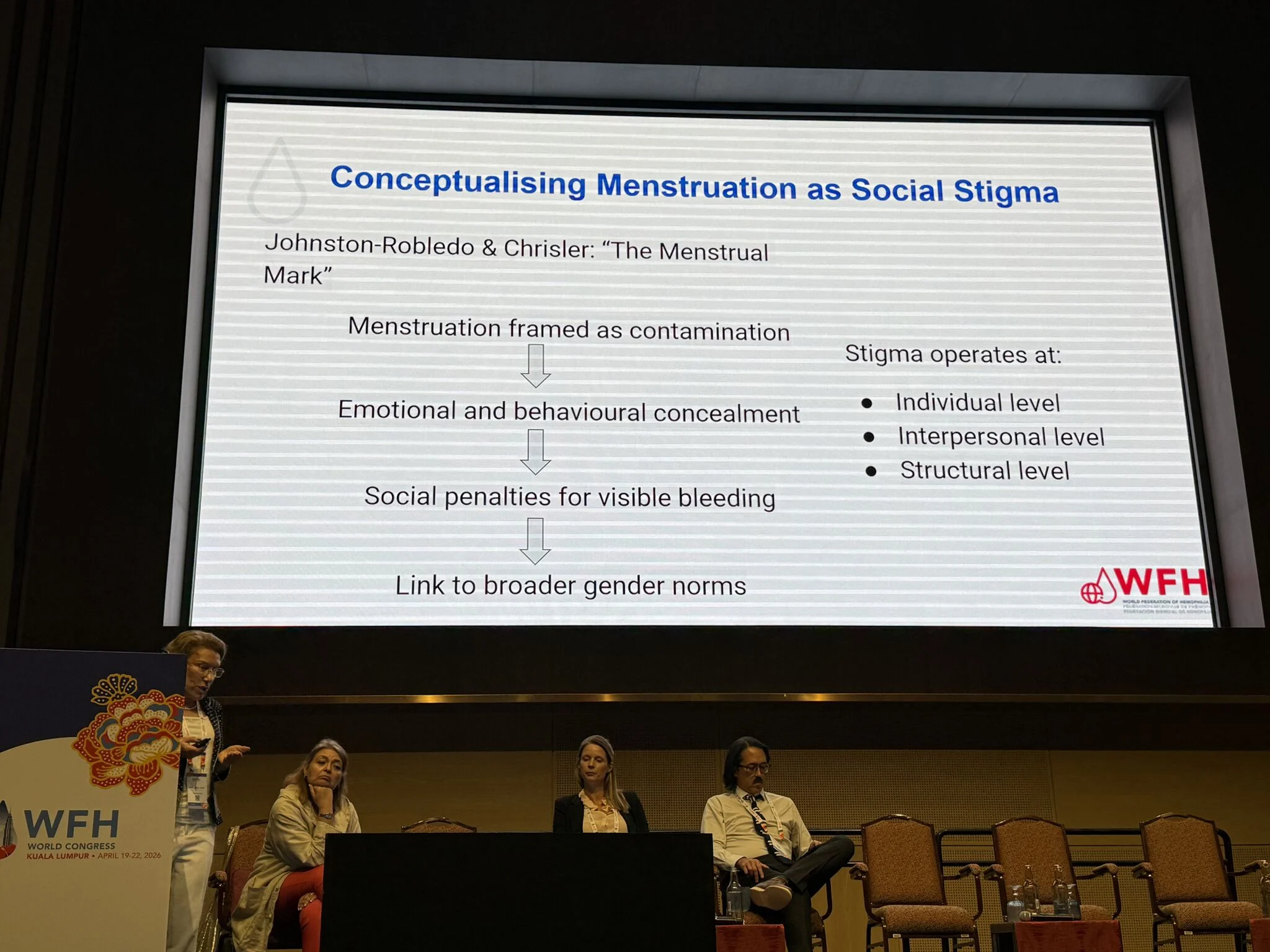
- From physiology to stigma-mediated pathology
Menstruation, while a universal biological process, is reframed across societies as taboo, impurity, or inconvenience. This sociocultural overlay transforms a clinical symptom (HMB) into a silenced condition, delaying presentation and masking underlying coagulopathies.
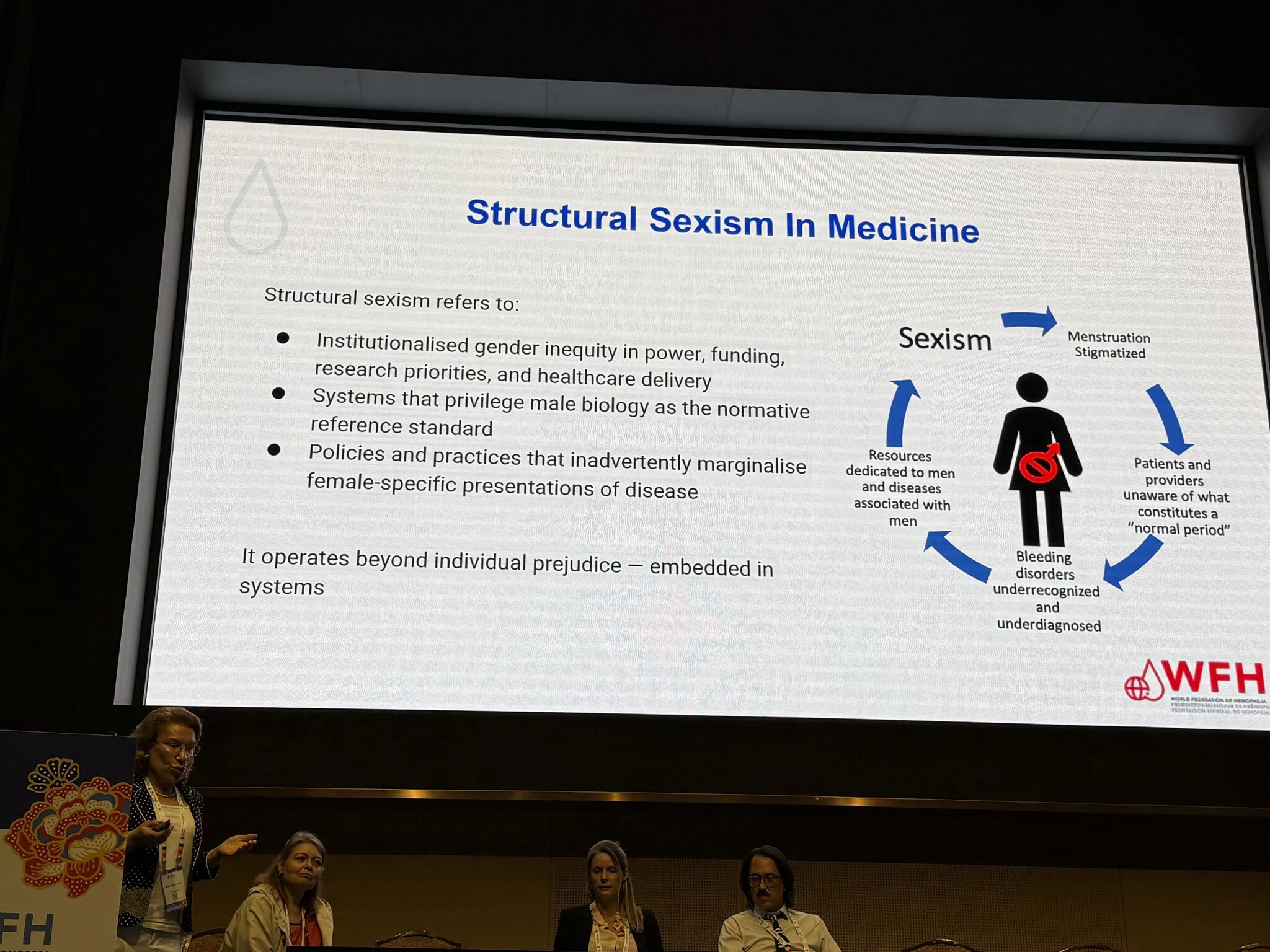
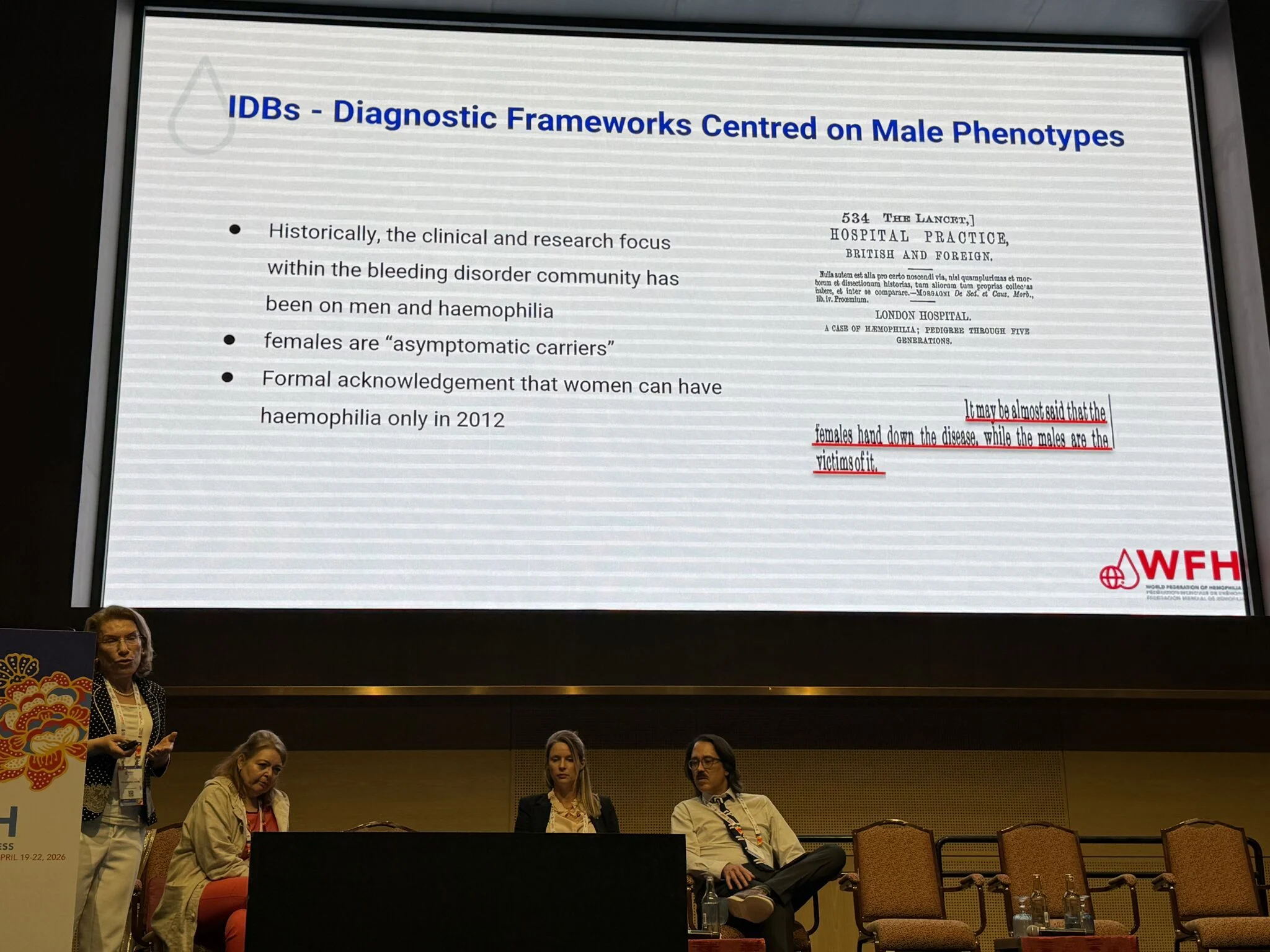
Structural sexism embedded in diagnostic paradigms
Modern hemostasis frameworks remain historically anchored in male phenotypes (hemophilia-centric models). As a result:
- Female bleeding symptoms are under-recognized
- Women are mislabeled as ‘carriers’ rather than patients
- Diagnostic thresholds fail to capture menstrual bleeding pathology
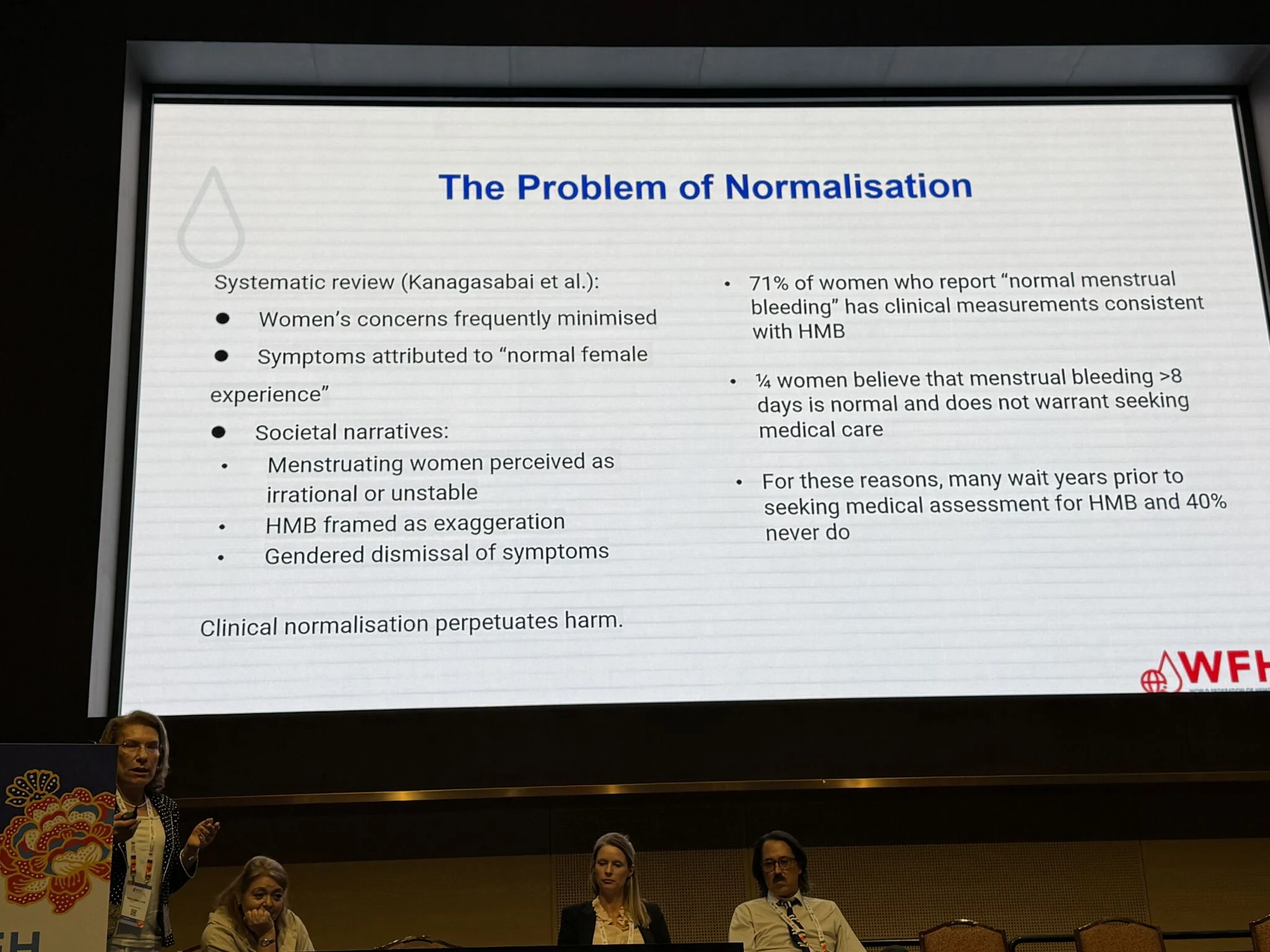
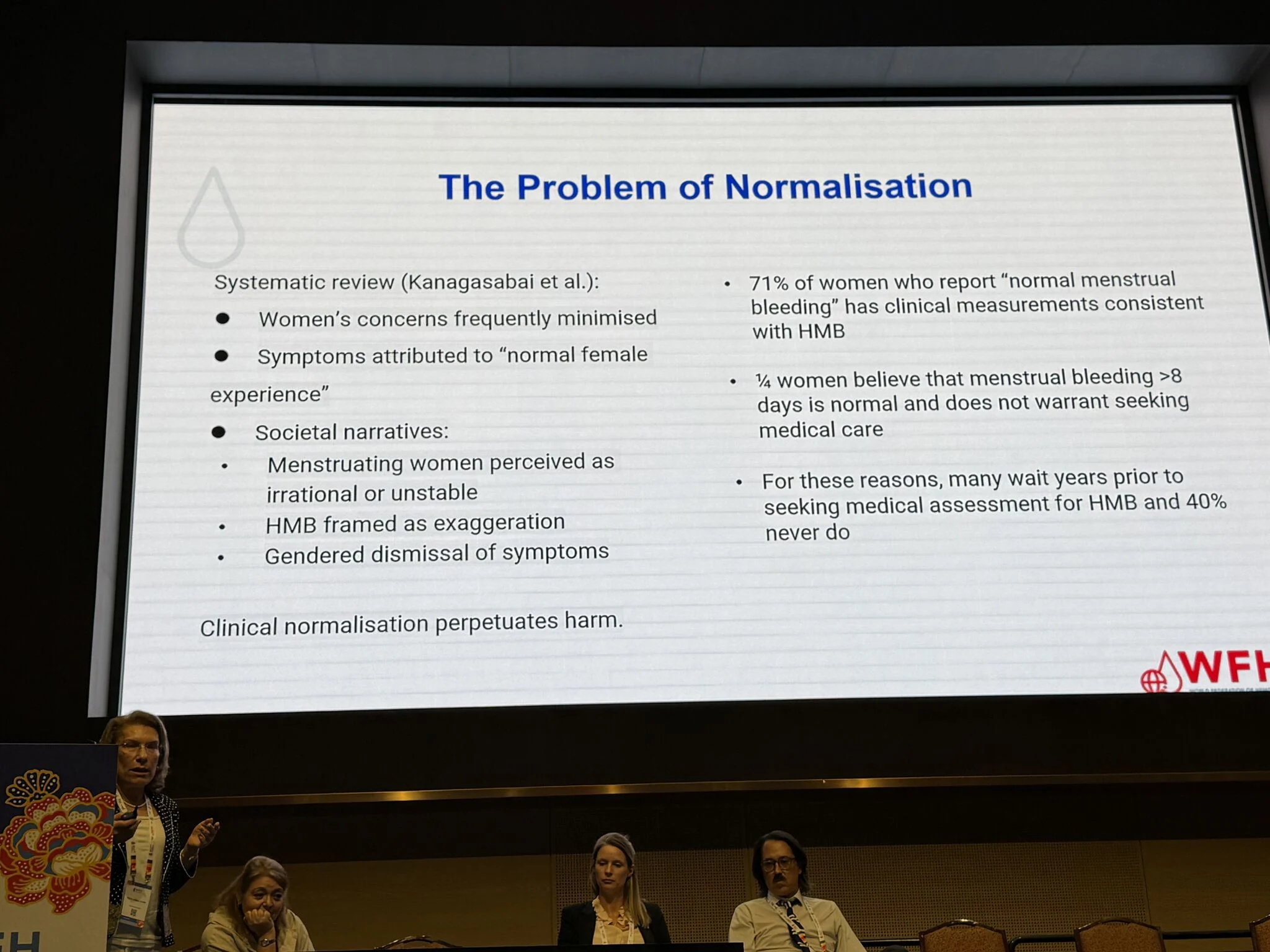
Normalization as a clinical risk factor
Data presented were striking:
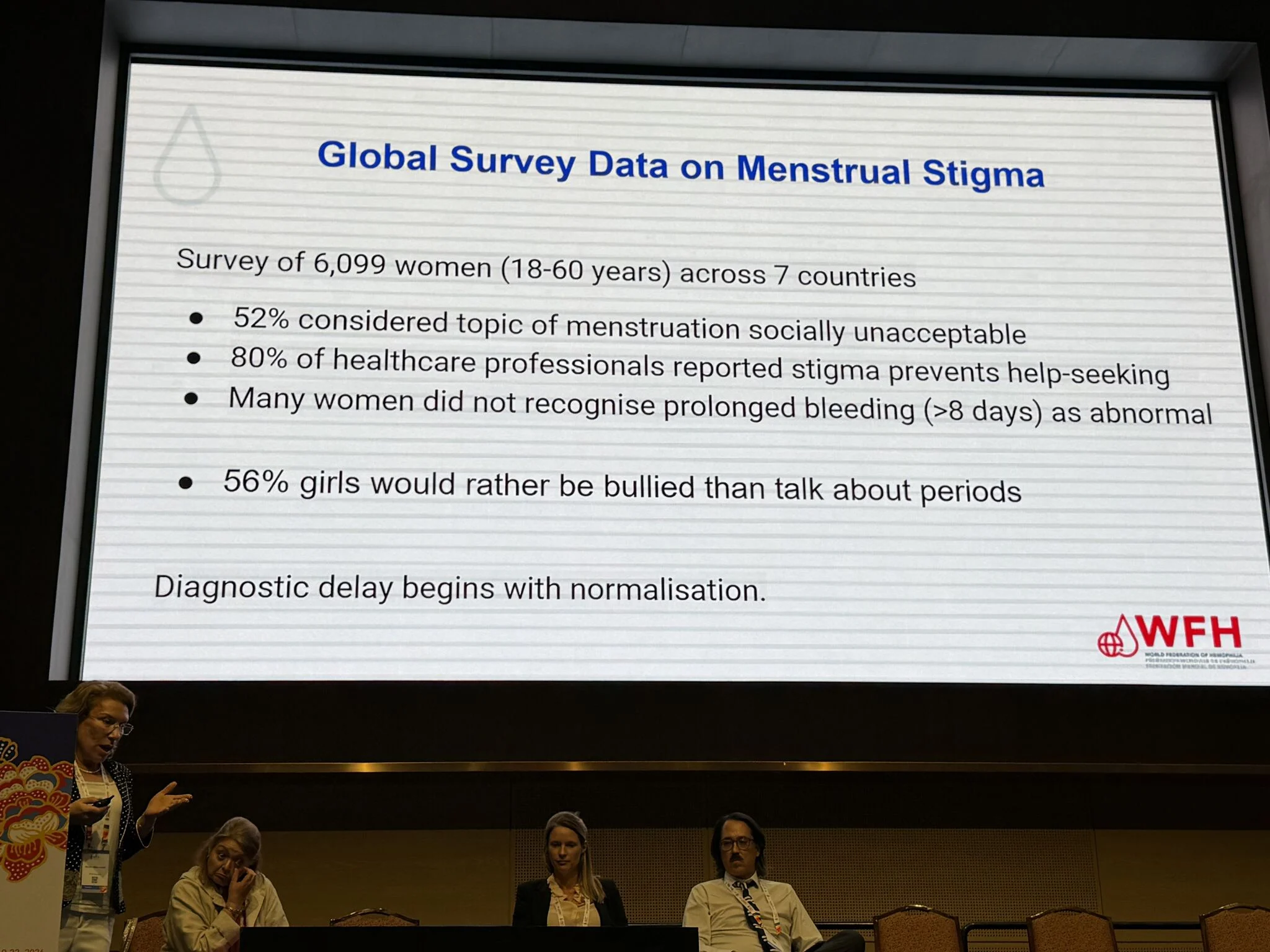
- Up to 71% of women with objectively defined HMB perceive their bleeding as ‘normal’
- A substantial proportion delay care for years, or never seek evaluation
This represents not lack of access—but distorted symptom perception shaped by societal narratives.
Stigma operates across three levels
- Individual: shame, concealment, internalized minimization
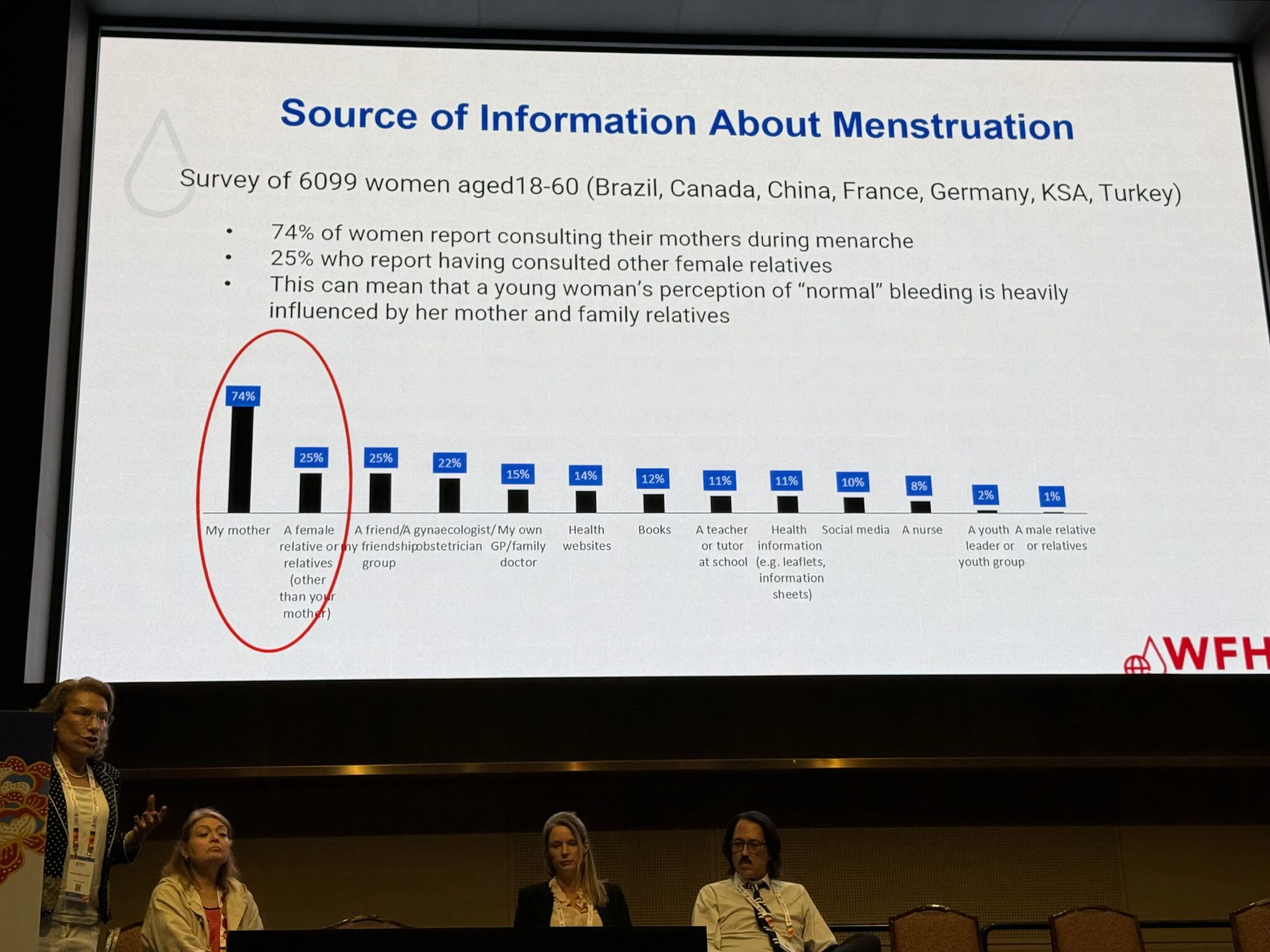
- Interpersonal: family influence (notably maternal normalization), cultural silence
- Structural: healthcare systems that deprioritize female-specific bleeding symptoms
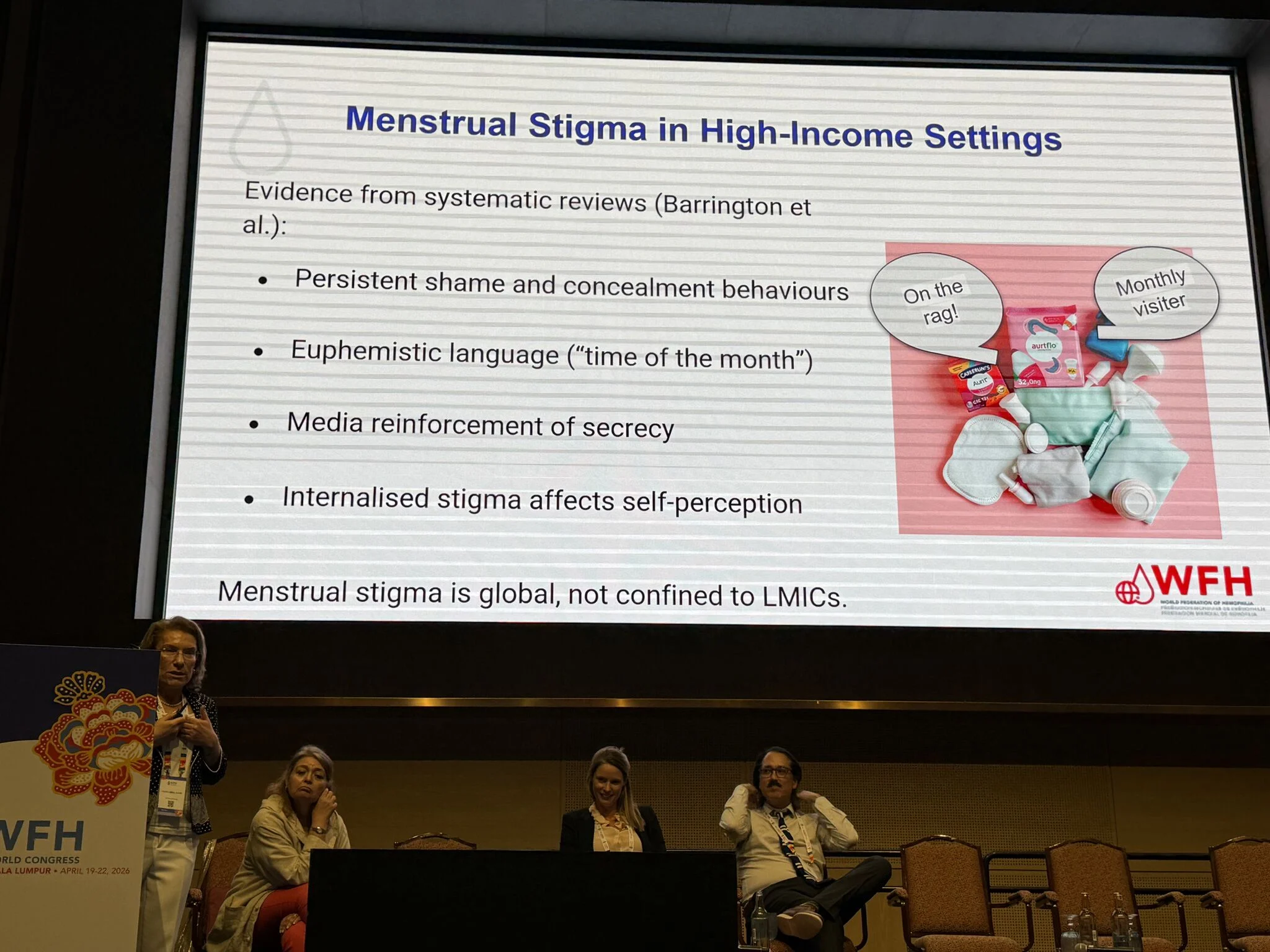
Global consistency of stigma
Importantly, menstrual stigma is not confined to LMICs. Evidence from high-income countries demonstrates persistent concealment behaviors, euphemistic language, and media-reinforced silence—indicating a universal epistemic gap in women’s health.
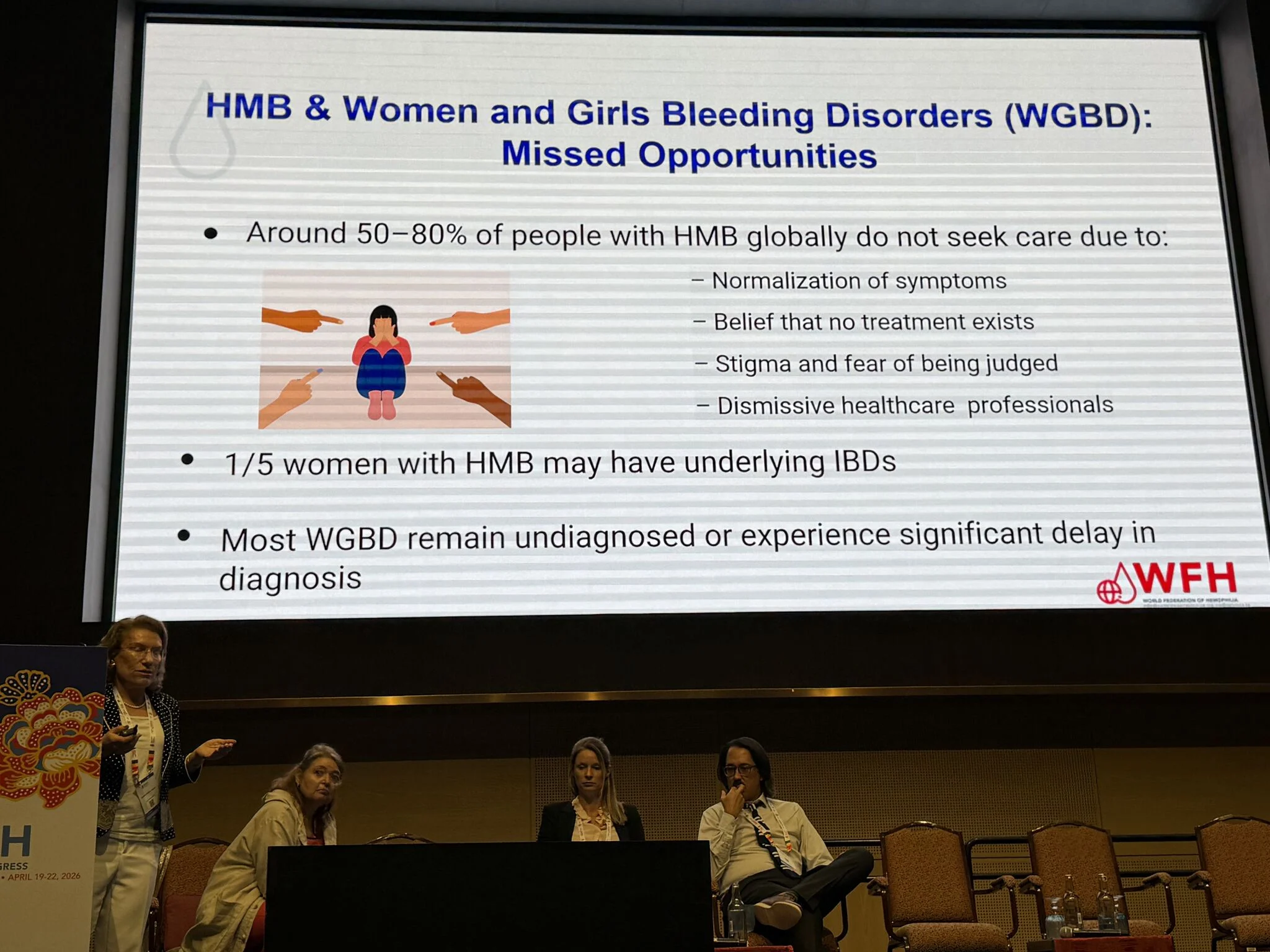
Missed diagnostic opportunities in HMB
- Up to 1 in 5 women with HMB may have an underlying bleeding disorder
- Yet 50–80% never seek care, largely due to stigma, normalization, and dismissive clinical encounters
Critical implication:
Diagnostic delay in women with bleeding disorders is not merely a clinical failure – it is a systemic failure of perception, language, and medical architecture.
To advance hemostasis care, we must:
- Reframe menstruation as a diagnostic signal, not a private inconvenience
- Integrate gender-sensitive diagnostic criteria
- Actively dismantle stigma within both society and healthcare systems
This session was not only informative – it was transformative, challenging us to reconsider how deeply social constructs shape clinical reality.”

See more in the gallery.
“From Stigma to System Failure: Why Women with Bleeding Disorders Remain Invisible
Building on the earlier discussion at the World Federation of Hemophilia Congress 2026, Rezan Abdul Kadir advanced the conversation from sociocultural stigma to operational and structural failures within healthcare systems.
Key systemic gaps and implications:
This variability creates diagnostic inconsistency across systems and countries.
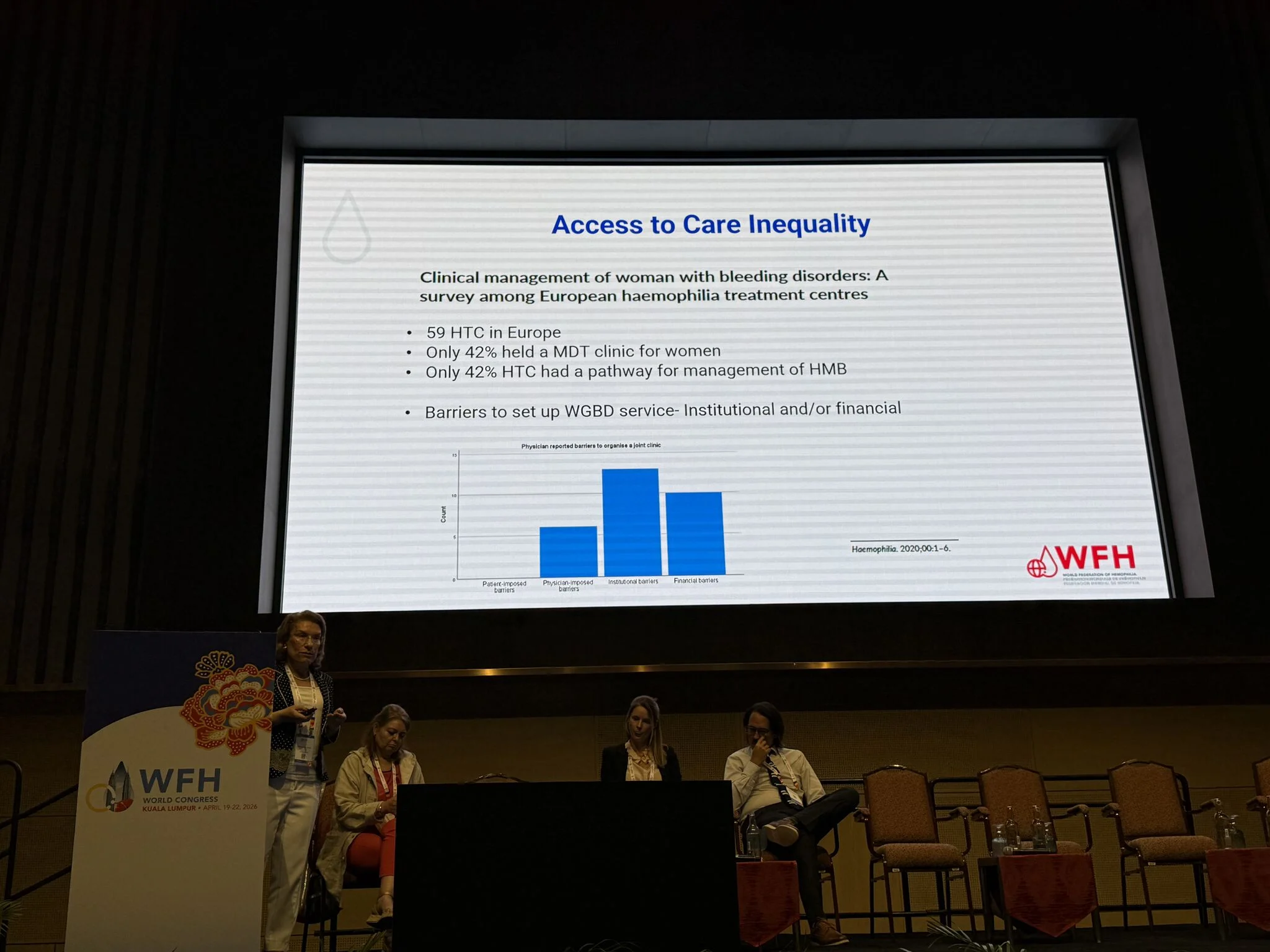
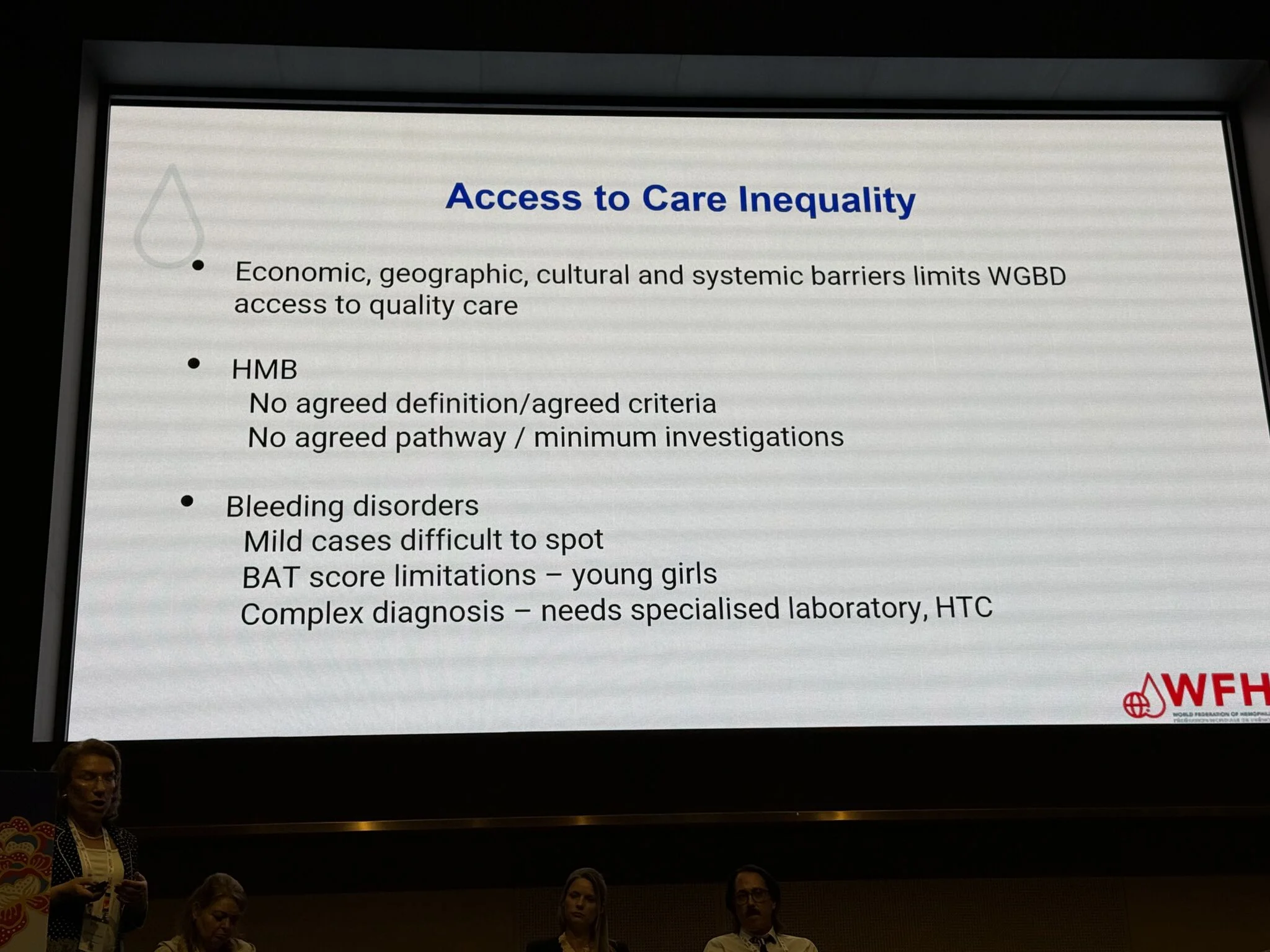
Access to care inequality as a multilayer barrier
Access is constrained by:
- Economic and geographic limitations
- Cultural barriers and stigma
- Lack of specialised centres (HTCs) and laboratory capacity
European data presented were particularly revealing:
- Only ~42% of haemophilia centres provide structured care pathways for women
- Multidisciplinary care models remain the exception, not the rule
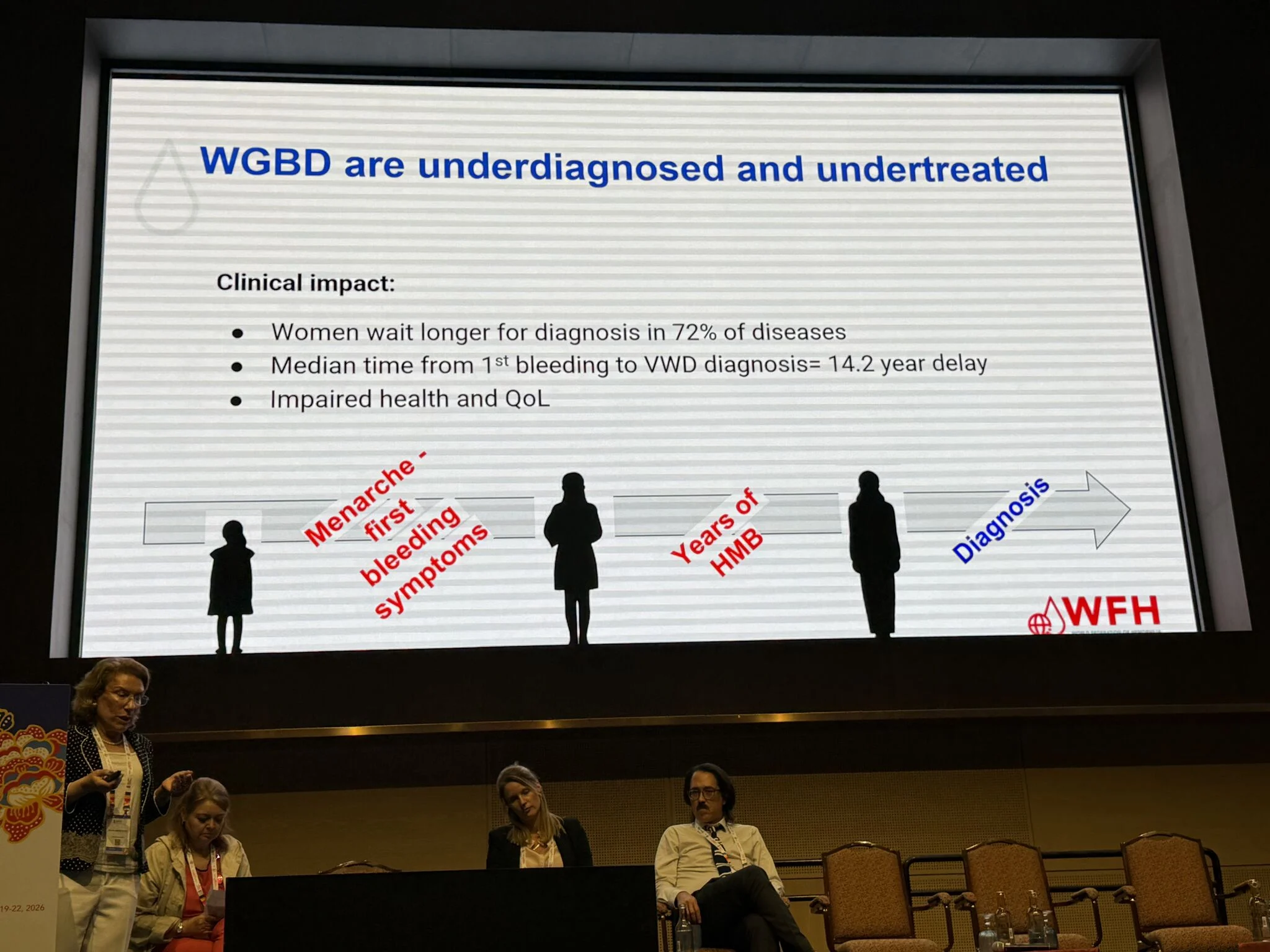
Diagnostic delay
- Women experience delayed diagnosis in ~72% of conditions
- Median delay to VWD diagnosis ≈ 14.2 years
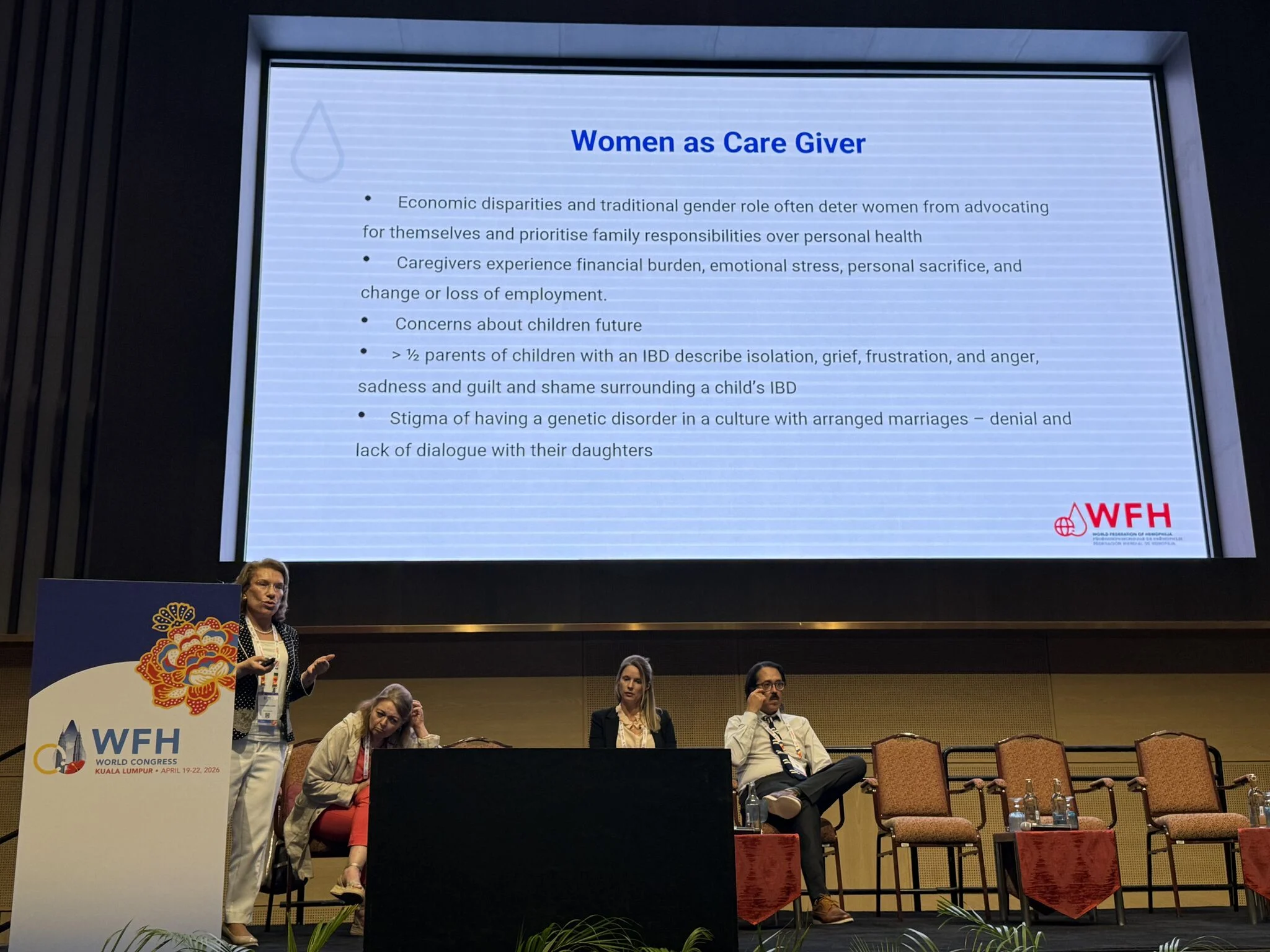
Gendered burden beyond the patient
This creates a feedback loop of silence, delay, and underdiagnosis across generations.
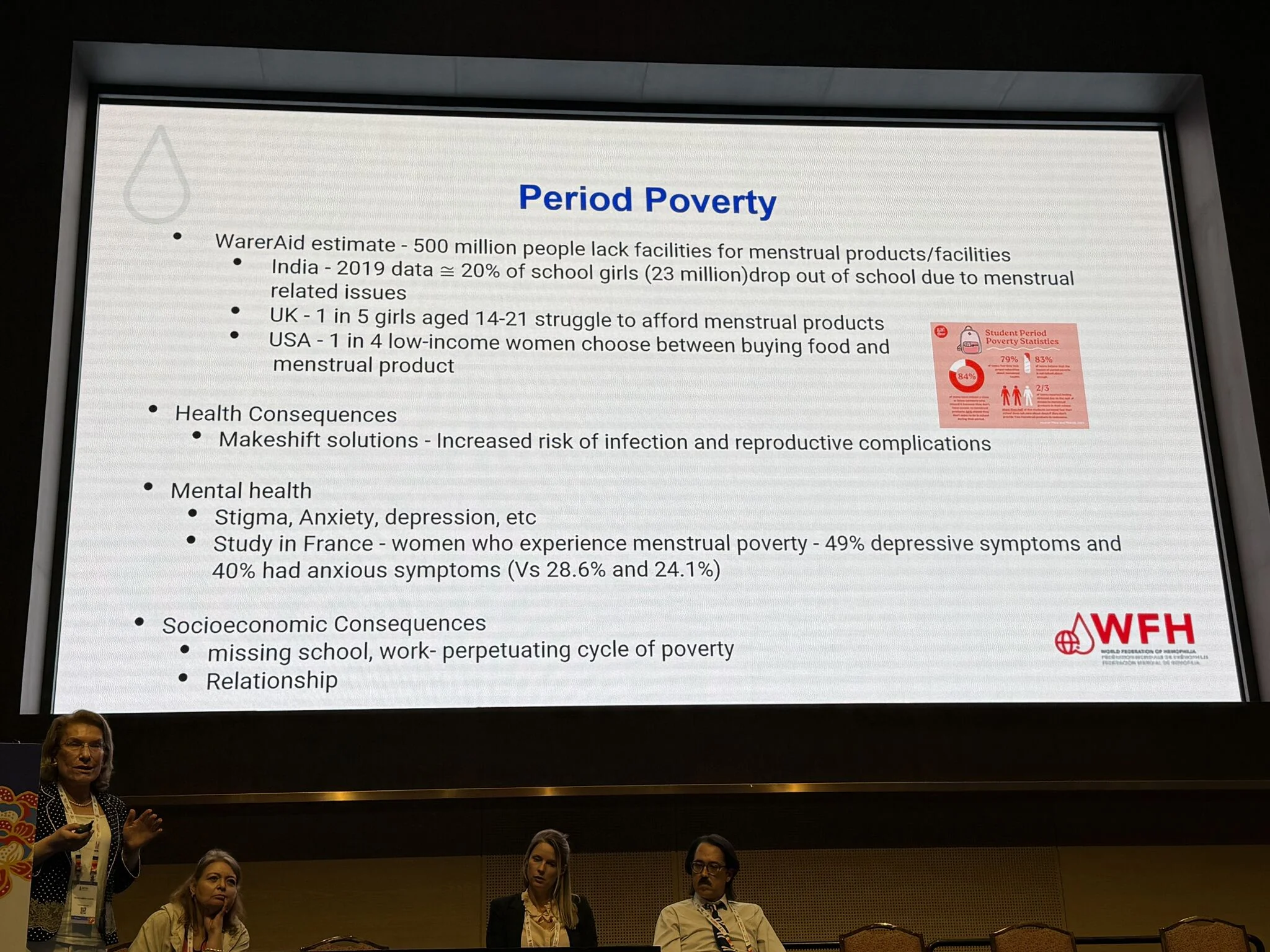
Period poverty as a clinical determinant
Menstrual health inequity is not only social – it is biomedical:
- Lack of access to menstrual products increases infection risk
- Leads to absenteeism, educational loss, and long-term socioeconomic impact
- Strong association with anxiety and depression
Period poverty should be recognised as a public health and hemostasis-relevant variable.
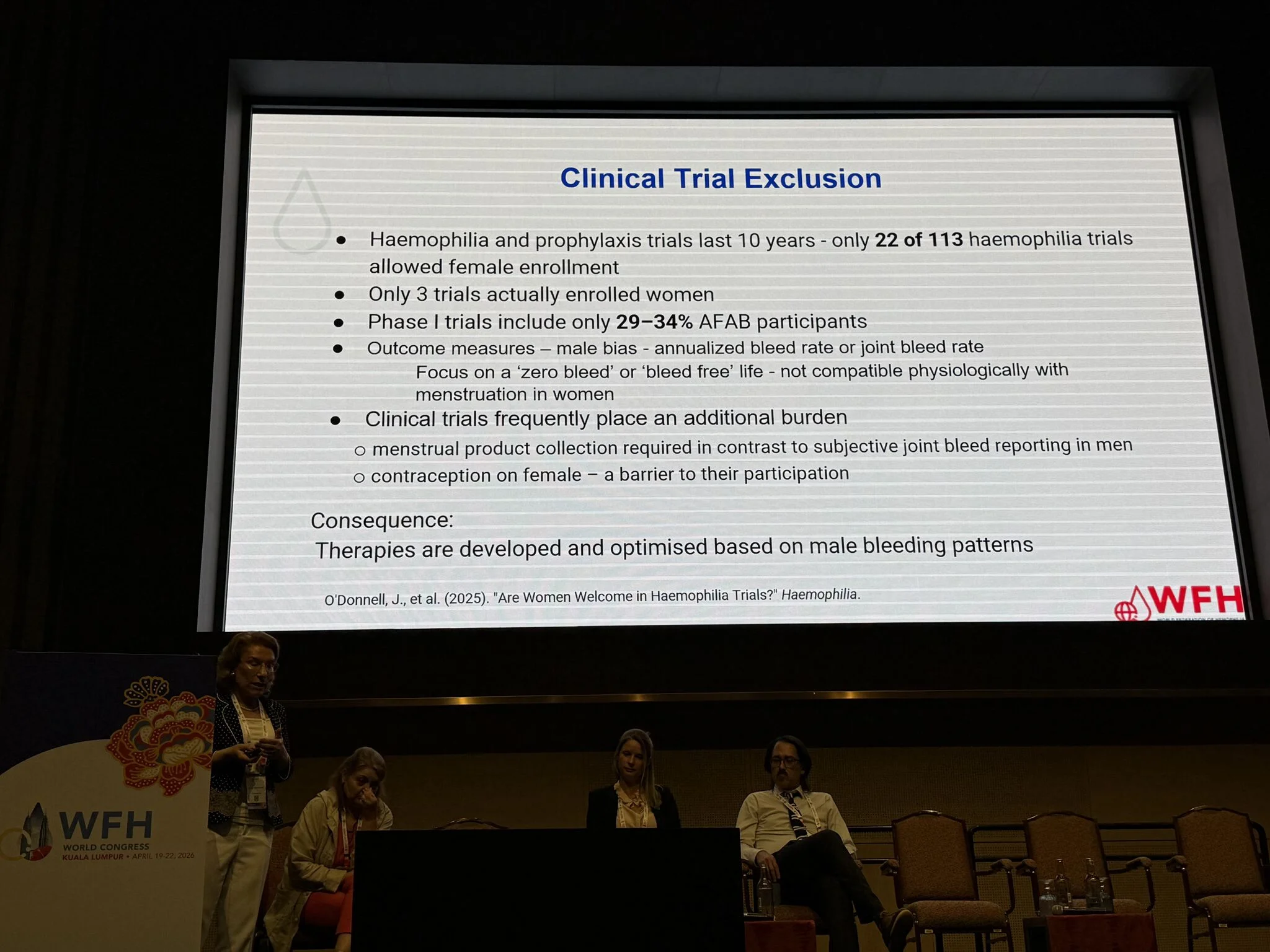
Exclusion from clinical trials: evidence bias at its core
The most striking structural issue:
- Only 22/113 hemophilia trials allowed female participation
- Minimal actual enrollment of women
- Outcome measures (e.g., annualized bleed rate) are male-centered
Therapies are therefore developed based on male bleeding phenotypes, limiting applicability to women.
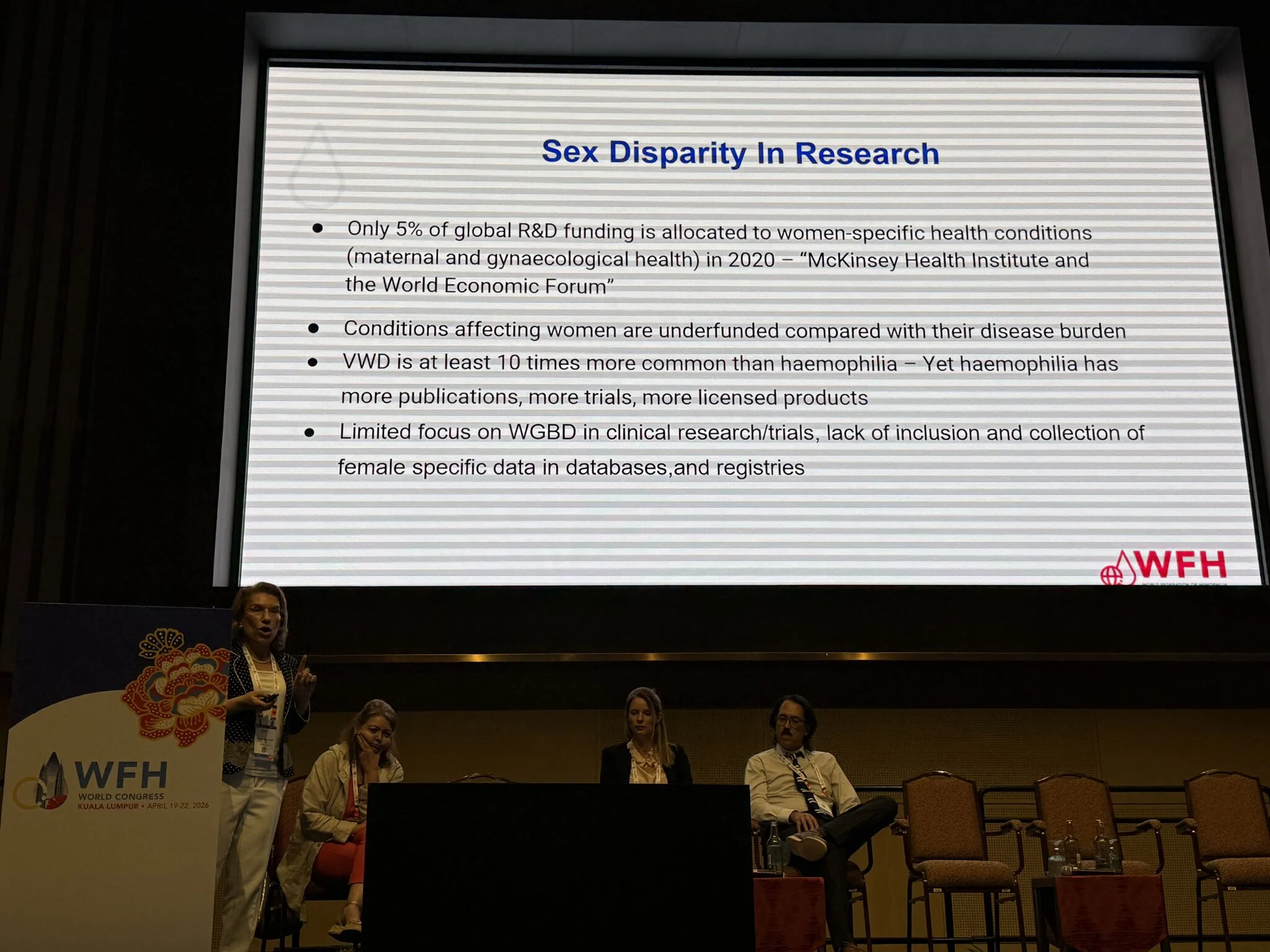
Sex disparity in research funding and focus
- Only ~5% of global R and D funding targets women-specific conditions
- VWD (more prevalent than hemophilia) remains under-researched
- Female-specific data are underrepresented in registries and trials
This creates a systematic evidence gap, reinforcing clinical invisibility.
Final analytical conclusion:
What begins as menstrual stigma evolves into a multi-layered systemic failure:
Strategic implications for hemostasis leadership:
- Rebuild diagnostic frameworks incorporating female-specific bleeding phenotypes
- Standardize HMB pathways and minimum investigation sets
- Expand HTC models to include multidisciplinary women-focused care
- Mandate female inclusion in clinical trials and registries
- Recognize menstrual health as a core component of bleeding disorder diagnostics
This session did not simply highlight disparities – it redefined them as structural, measurable, and actionable failures within modern medicine.”

See more in the gallery.
“Beyond Awareness: Measuring What We Miss in Women’s Bleeding Disorders
At the World Federation of Hemophilia Congress 2026, Joanna Davies delivered a compelling analysis on why HMB remains systematically underestimated—and how digital innovation may change that.
Key insights:
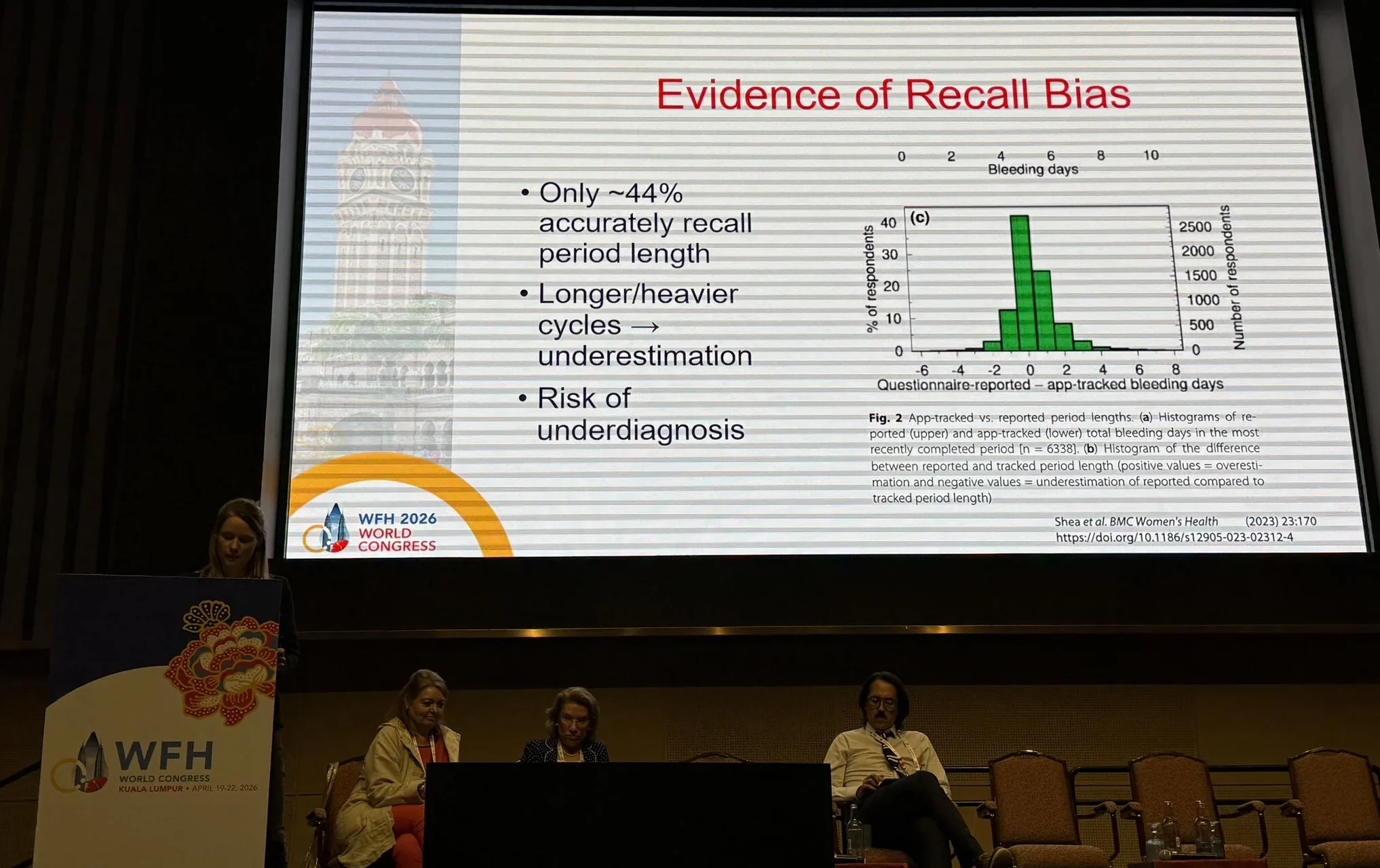
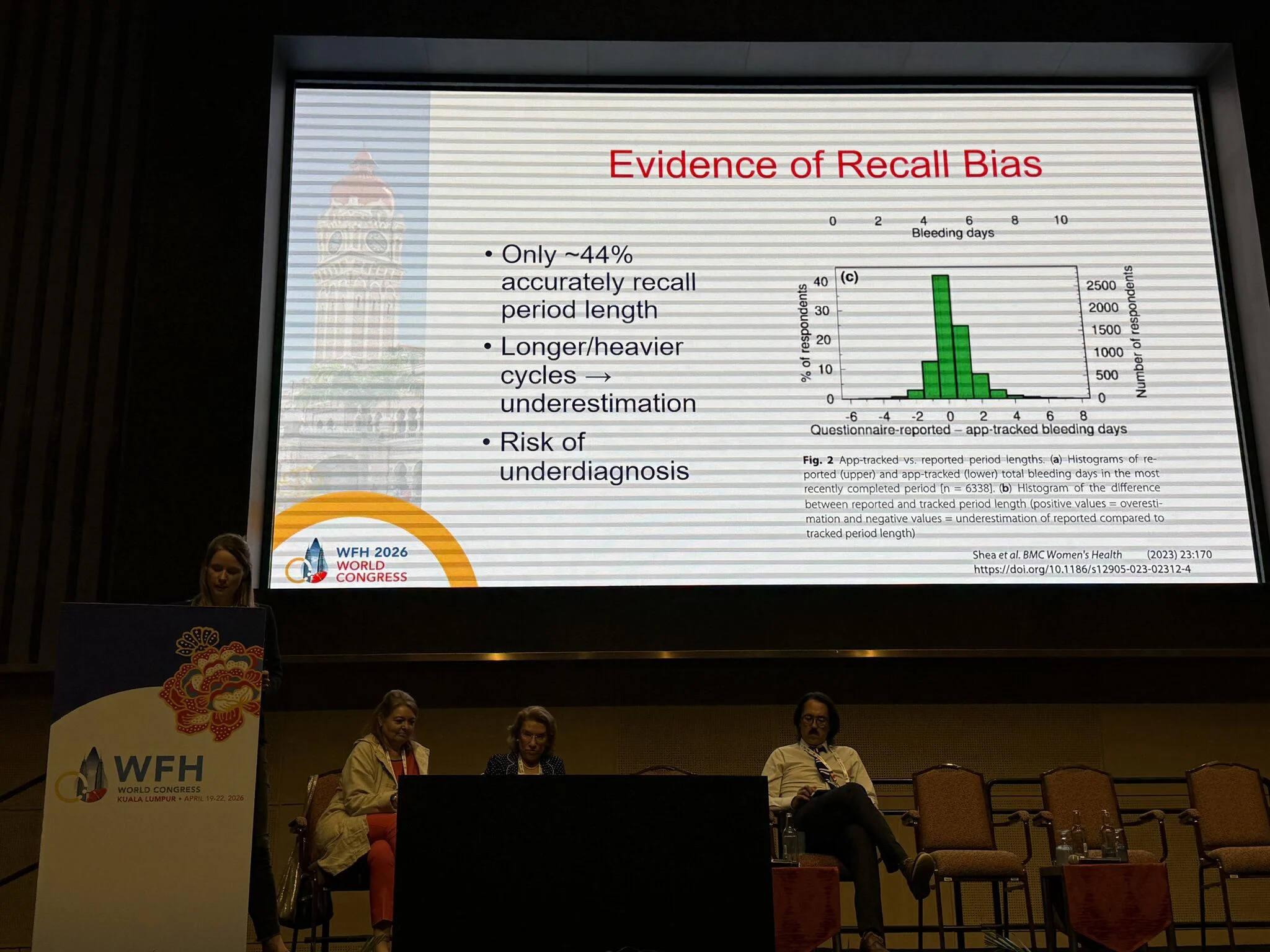
- Recall bias is clinically relevant
Only ~44% of women accurately recall menstrual duration.
Heavier cycles lead to systematic underestimation, leading to missed diagnosis.
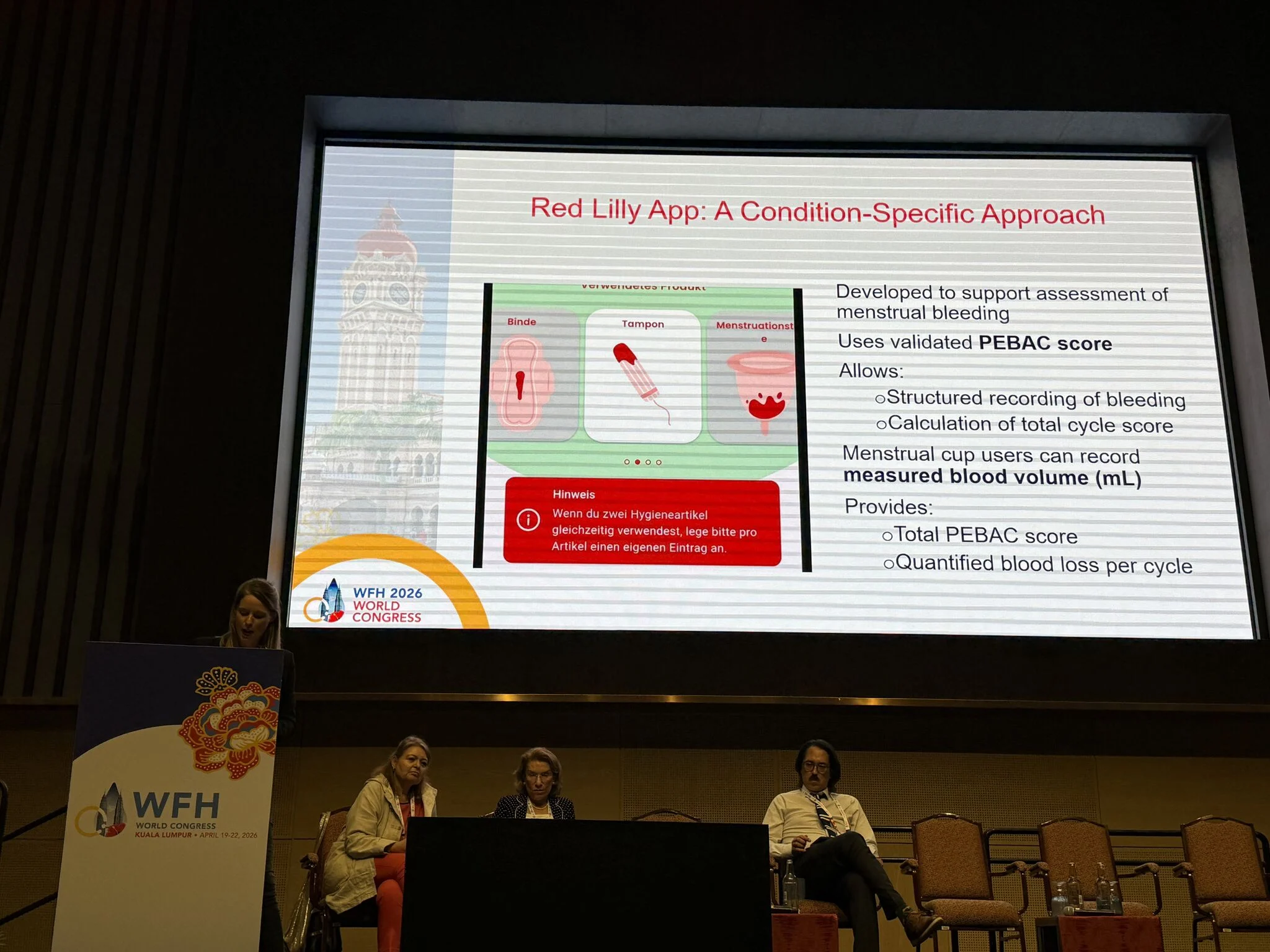
- From subjective to objective metrics
Tools like PBAC/PEBAC-based apps (e.g., WeThrive, RedLilly) enable:
- structured bleeding quantification
- cycle-level scoring
- real-world data capture
Bridging the gap between symptoms and diagnosis.
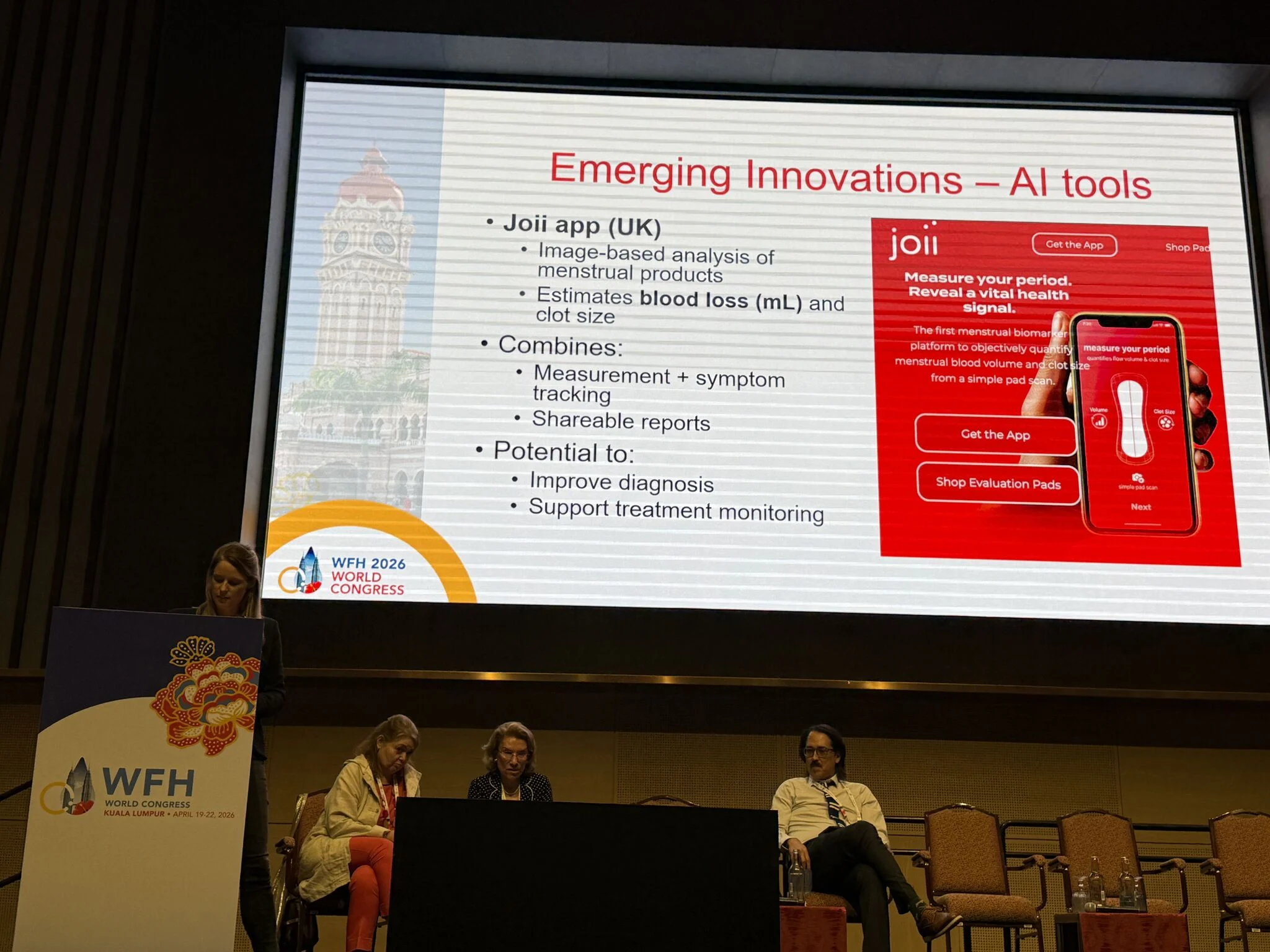
- AI-driven innovation
Emerging tools (e.g., Joii app) use image-based analysis to estimate blood loss and clot burden.
Potential to transform HMB into a measurable biomarker.
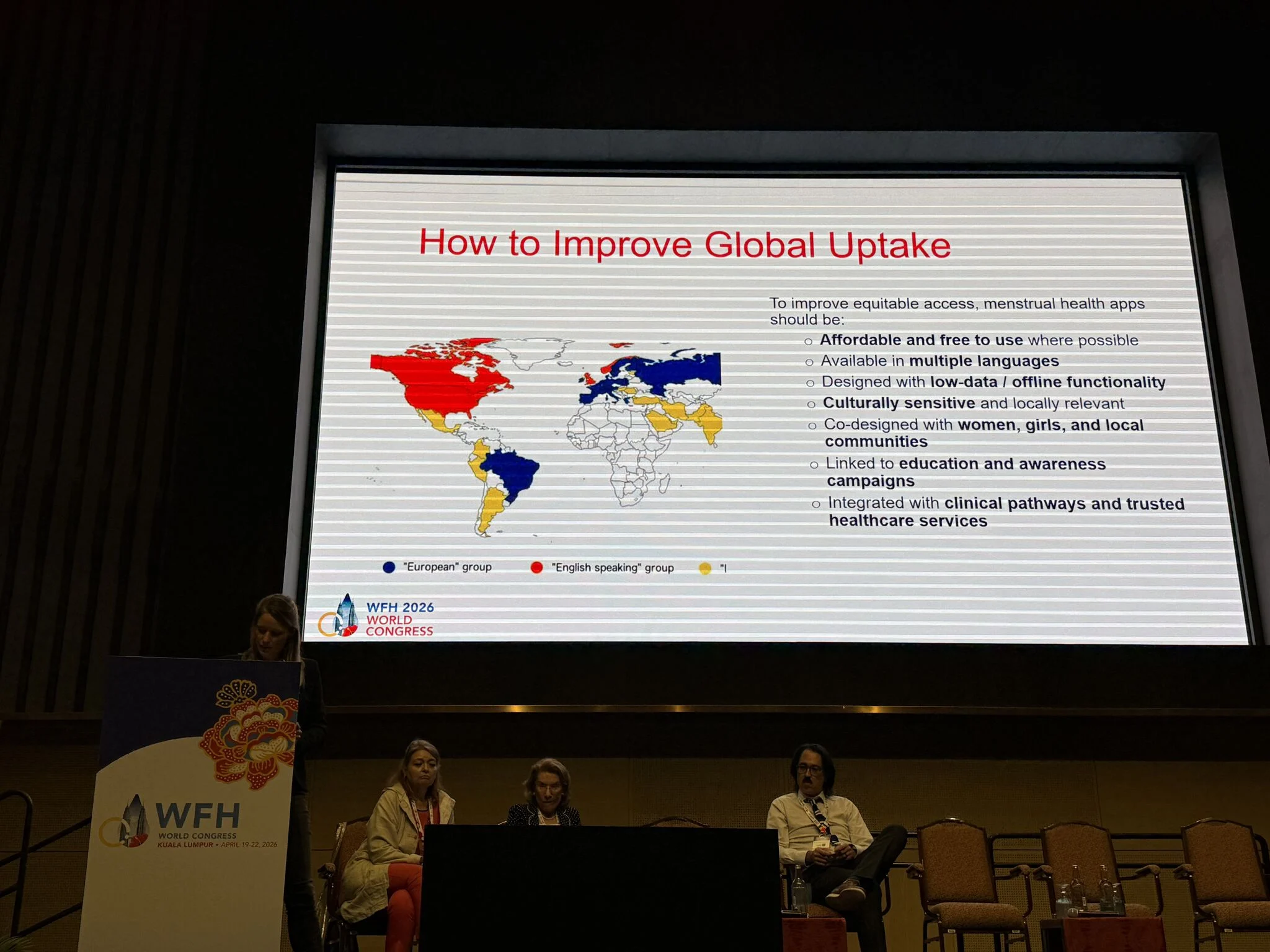
Equity challenges persist
Digital health is not neutral:
- cost, literacy, language
- cultural stigma
- data privacy concerns
Digital access is becoming a determinant of health.
- Trust and regulation matter
- Adoption depends on transparency, data protection frameworks (e.g., GDPR), and cultural acceptability.
Conclusion:
From recall bias to data capture to clinical integration
We are entering an era where measurement can correct inequity.
Final note:
The session was elegantly closed by Emma Goudemand, who notably thanked the minority of men present in the audience – a subtle but powerful reflection of the gender imbalance this field still faces.”

See more in the gallery.
Stay up-to-date with the latest advancements in hematology through Hemostasis Today.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-
Aug 11, 2026, 05:53Isaac Okello: Strengthening Sickle Cell Advocacy in Uganda
-
Aug 11, 2026, 05:38Rami Unterman: A Simple New Biomarker for Fibrotic ILDs
-
Aug 11, 2026, 04:10Haroun Gajraj: CLaCS vs Sclerotherapy – What Does the Evidence Show
-
Aug 11, 2026, 02:54Tareq Abadl: The Ultimate Guide to Clinically Significant Antibodies
-
Aug 10, 2026, 17:35Chokri Ben Lamine: Balancing Holistic Care and Precision in Hematology
-
Aug 10, 2026, 17:14Anna Stanizzi: Patient Blood Management as a New Model of Personalized Care
-
Aug 10, 2026, 17:12Odong Christopher: New Research on Ischemic Stroke Prediction in Uganda
-
Aug 10, 2026, 16:58Jeff Szer AM: Advancing the Management of Paroxysmal Nocturnal Hemoglobinuria
-
Aug 10, 2026, 16:51Suebsarn Ruksakulpiwat։ A New Milestone in the Development of the Stroke Risk Screening Scales