

Mazou Ngou Temgoua: Cancer and VTE – Toward Truly Personalized Anticoagulation
Mazou Ngou Temgoua, Cardiology Intensive Care Physician at Châteauroux–Le Blanc Hospital Centre, shared a post on LinkedIn about recent article by Faizan Khan et al., published in European Heart Journal:
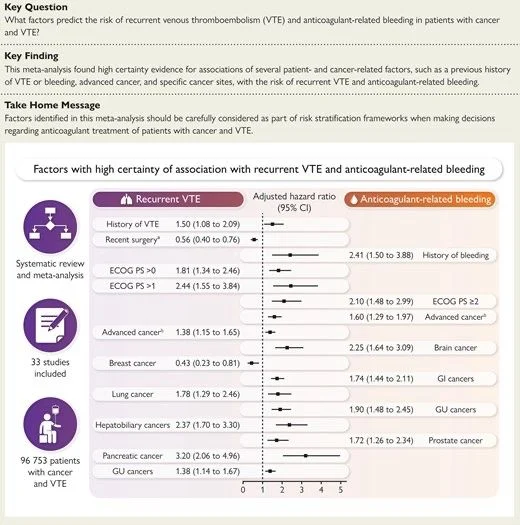
“Cancer and VTE: toward a truly personalized (and finally nuanced) anticoagulation
A major meta-analysis (>96,000 patients) provides a key message:
- Not all cancers expose thrombosis vs bleeding to the same balance
- And above all, the profiles are not symmetrical
What the study really shows: getting out of shortcuts
High thromboembolic risk (without necessarily increased bleeding) (e.g. pancreas, hepatobiliary, lung, history of VTE, ECOG >0)
- Dominant pro-thrombotic profile
High bleeding risk (without clear evidence of reduced VTE risk) (e.g. gastrointestinal cancers [non-pancreas/hepatobiliary], brain, prostate, history of bleeding, ECOG ≥2)
- Dominant haemorrhagic profile
- But thrombotic risk is not necessarily low
High dual risk (critical profile) (e.g. cancers of the genitourinary tract, advanced cancer and deterioration of general condition)
- High risk of recurrence and bleeding
Lower risk of recurrence (e.g. recent surgery, breast cancer)
- More favourable profile
- To be recontextualized according to tumor activity
Major implication: reasoning in terms of risk dominance (not simplistic categories)
Dominant thrombotic profile
- Prolonged, intensive anticoagulation (greater than or equal to 6 months, no early reduction)
Dominant bleeding profile
- Cautious, individualized anticoagulation
- Not necessarily short, but adapted to the real context of VTE
High dual risk (the real challenge)
- No standard solution
- Tailor-made strategy:
- LMWH preferred
- Close reassessment
- Multidisciplinary discussion
- Shared decision-making
Lower risk profile (relative)
- Standard anticoagulation
- If active cancer, tendency to still prolong treatment (greater than or equal to 6 months)
What this study really changes
Breaks the simplistic opposition ‘high risk vs low risk’
Shows that some cancers are:
- Purely thrombogenic (pancreas)
- More haemorrhagic (digestive, brain)
- Or mixed (genitourinary)
Bleeding risk does not equal protection against recurrence
Important limitations
Heterogeneity of studies
- Combined factors not assessed
- Absence of biomarkers
- Current scores insufficient
- Uncertain applicability after the acute phase
Key message (essential takeaway)
- The real advance is not to add risk factors
- But to understand their interaction and clinical dominance
Anticoagulation in cancer becomes:
- Dynamic
- Personalized
- Patient-centred
Future progress will require integrated models (clinical, biomarkers, and artificial intelligence) to manage these complex profiles.”
Title: Predictors of recurrent venous thromboembolism and bleeding in patients with cancer: a meta-analysis
Authors: Faizan Khan, Tobias Tritschler, Caterina E. Marx, Vincent Lanting, Bram Rochwerg, Alexandre Tran, Shannon M. Fernando, Diane L. Lorenzetti, Hannah Wunsch, Jessalyn Holodinsky, Kirsten Fiest, Henry Thomas Stelfox, Aurélien Delluc, Dean A. Fergusson, Grégoire Le Gal, Philip S. Wells, Tzu-Fei Wang, Kristen Sanfilippo, Nick van Es, Deborah Schrag, Jean M. Connors, Marc Carrier

Stay updated with Hemostasis Today.
{kind=link}
-
Jul 26, 2026, 13:32Ahmed Kotb: A Practical Guide to Von Willebrand Disease
-
Jul 26, 2026, 12:42Emmanuel J Favaloro: Celebrating Excellence in Scientific Peer Review
-
Jul 26, 2026, 12:20Advancing Sickle Cell Care Through Advocacy – American Society of Hematology
-
Jul 26, 2026, 12:04Paolo Zamboni: Marking 50 Years in Medicine
-
Jul 26, 2026, 11:55William Wallace: Muscle Aging Emerges as the Strongest Mortality Predictor
-
Jul 26, 2026, 08:51Dayita Banerjee: Presenting New Insights in Fibrinolysis Research at ISTH 2026
-
Jul 26, 2026, 08:39Roshni Kulkarni: The Human Face of Postpartum Hemorrhage
-
Jul 26, 2026, 08:14Atahar imam Hasan: Universal Artificial Blood and the Future of Trauma Care
-
Jul 26, 2026, 07:40Maha Othman: Leading Scientific Collaboration Across Hemostasis at ISTH 2026