
Elias Lee: Acute PE from Subclavian VT – CT Scan Diagnosis, Radiology Interpretation, and Emergency Imaging Insights
Elias Lee, Professor at Nambu University, shared a post on LinkedIn:
“Introduction: A Silent Threat in Emergency Diagnosis
A 42 year old patient arrives at the emergency department with sudden dyspnea and mild chest discomfort.
Vital signs are borderline unstable. Initial chest X – ray is unremarkable.
However, within minutes, a CT pulmonary angiography (CTPA) reveals a life – threatening condition: acute pulmonary embolism (PE) originating from subclavian venous thrombosis.
This scenario highlights the critical importance of CT scan diagnosis, radiology interpretation, and increasingly, medical imaging AI in modern trauma imaging and emergency diagnosis workflows.
Pulmonary embolism remains one of the most underdiagnosed yet potentially fatal conditions in acute care medicine.
When the embolic source is atypical – such as the upper extremity venous system (subclavian vein) – diagnostic complexity increases significantly.
Pathophysiology of Acute Pulmonary Embolism
Pulmonary embolism occurs when thrombotic material – typically originating from the venous system – travels through the right heart into the pulmonary arterial circulation.
Mechanism of Thrombus Formation
The development of subclavian venous thrombosis follows Virchow’s triad:
- Endothelial injury
- Venous stasis
- Hypercoagulability
In upper extremity veins, common triggers include:
- Central venous catheter placement
- Repetitive arm motion (effort thrombosis, Paget – Schroetter syndrome)
- Thoracic outlet compression
- Malignancy – associated thrombosis
Embolization Process
Once dislodged:
- Thrombus travels via: Subclavian vein – Brachiocephalic vein – Superior vena cava
- Reaches: Right atrium – Right ventricle
- Lodges in: Pulmonary arteries
This results in:
- Increased pulmonary vascular resistance
- Right ventricular strain
- Impaired oxygenation
Epidemiology
Although most pulmonary emboli originate from lower extremity deep veins, upper extremity sources account for:
- nearly 10–15% of all DVT cases
- Increasing incidence due to: Central venous devices, Oncology patients, and ICU interventions
High – Risk Populations
- Cancer patients
- ICU patients with catheters
- Athletes with repetitive upper limb activity
- Post – surgical patients
Clinical Presentation
Symptoms can be subtle and misleading.
Common Symptoms
- Sudden dyspnea
- Chest pain (pleuritic)
- Tachycardia
- Hypoxia
Upper Extremity Clues
- Arm swelling
- Dilated superficial veins
- Shoulder discomfort
Red Flags in Emergency Diagnosis
- Unexplained hypoxia
- Syncope
- Hemodynamic instability
Imaging Features: The Role of CT Scan Diagnosis
Why CT Pulmonary Angiography (CTPA)?
CTPA is the gold standard in radiology interpretation for PE due to:
- High sensitivity and specificity
- Rapid acquisition
- Ability to assess alternative diagnoses

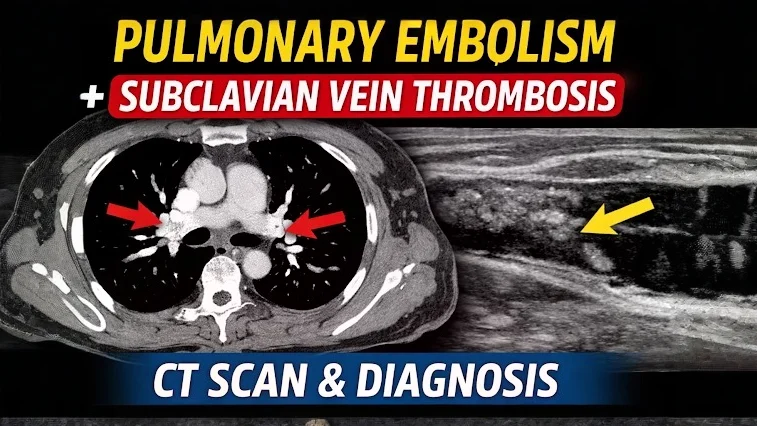
Figure 1. Axial Contrast – Enhanced CT of the Thoracic Inlet
This axial contrast – enhanced CT image at the level of the thoracic inlet demonstrates an intraluminal filling defect within the subclavian vein, consistent with acute subclavian venous thrombosis.
Key Radiologic Findings:
- The affected subclavian vein appears partially opacified, with a central low – attenuation (hypodense) filling defect, indicating thrombus.
- There is asymmetry compared to the contralateral side, where the vein is normally enhanced with contrast.
- Mild venous distension may be present, suggesting acute obstruction.
- Surrounding soft tissues may show subtle edema, supporting an acute process.
Clinical Significance:
These findings confirm upper extremity deep vein thrombosis (UEDVT) involving the subclavian vein.
This is a clinically important source of pulmonary embolism, particularly in patients with risk factors such as central venous catheterization or thoracic outlet syndrome.
Early detection on CT is critical for prompt anticoagulation and prevention of embolic complications.
Diagnostic Contribution:
This image plays a key role in:
- Identifying the primary thrombotic source
- Supporting the diagnosis of thromboembolic disease
- Guiding further evaluation for pulmonary embolism via CT pulmonary angiography

Figure 2. Axial Contrast – Enhanced CT Pulmonary Angiography (CTPA)
This axial contrast – enhanced CT image of the chest demonstrates a filling defect within the pulmonary arterial system, consistent with acute pulmonary embolism.
Key Radiologic Findings:
- A hypodense intraluminal filling defect is seen within a contrast – opacified pulmonary artery (likely at the lobar or segmental level).
- The thrombus is surrounded by contrast material, producing the classic ‘Polo mint sign’ (central defect with peripheral contrast)
- The involved artery may appear slightly expanded, suggesting an acute process.
- The adjacent lung parenchyma appears relatively preserved, without clear infarction in this slice.
Clinical Significance:
- This image confirms the diagnosis of acute pulmonary embolism (PE).
- In the context of subclavian venous thrombosis (Figure 1), this represents a proximal embolic complication.
- Acute PE can lead to: Increased pulmonary vascular resistance, right ventricular strain, and potential hemodynamic instability
Diagnostic Contribution:
This figure is critical for:
- Establishing a definitive CT scan diagnosis of pulmonary embolism
- Demonstrating the direct intravascular clot rather than indirect signs
- Supporting urgent initiation of anticoagulation or thrombolytic therapy
Radiology Insight (Expert Level):
- Acute emboli typically form acute angles with the vessel wall
- Chronic emboli (not seen here) would show: Eccentric location, Wall – adherent thrombus, Possible calcification

Figure 3. Coronal Contrast – Enhanced CT Pulmonary Angiography (CTPA)
This coronal reformatted contrast – enhanced CT image demonstrates extensive intraluminal filling defects within the central pulmonary arterial system, consistent with acute pulmonary embolism.
Key Radiologic Findings:
- A large hypodense filling defect is visualized within the main pulmonary artery extending into the right and/or left pulmonary arteries.
- The thrombus is surrounded by contrast, clearly delineating the embolus.
- The clot appears to bridge across the pulmonary artery bifurcation, raising suspicion for a:Saddle pulmonary embolism
- There is a partial obstruction of blood flow to both lungs.
- Peripheral pulmonary arterial branches may show reduced opacification.
Clinical Significance:
- This represents a high clot burden pulmonary embolism, which is clinically significant and potentially life – threatening.
- Saddle emboli are associated with: Increased risk of right ventricular failure, higher likelihood of hemodynamic instability
- In the context of prior findings (e.g., subclavian vein thrombosis), this confirms embolic propagation from a proximal venous source.
Diagnostic Contribution:
This image is crucial for:
- Assessing the extent and distribution of emboli
- Identifying central (proximal) embolism, which has a greater clinical impact than peripheral emboli
- Supporting risk stratification and urgent treatment decisions
Radiology Insight (Expert Level):
- Coronal reconstructions are particularly useful for: Visualizing longitudinal clot extent, detecting saddle emboli
- Acute emboli typically: Form central filling defects, expand the vessel
- Chronic emboli (not suggested here) would show: Eccentric wall-adherent thrombusVessel narrowing or webs

Figure 4. Sagittal Contrast – Enhanced CT Pulmonary Angiography (CTPA)
This sagittal reformatted contrast – enhanced CT image of the chest demonstrates a filling defect within the pulmonary arterial system, consistent with acute pulmonary embolism, along with parenchymal changes suggestive of pulmonary infarction.
Key Radiologic Findings:
- A hypodense intraluminal filling defect is seen within a pulmonary arterial branch, indicating embolic thrombus.
- The surrounding contrast outlines the clot, confirming intraluminal obstruction.
- There is a peripheral, wedge – shaped area of increased attenuation in the adjacent lung parenchyma. This appearance is characteristic of pulmonary infarction.
- The lesion is located in a dependent posterior region, which is typical for embolic infarcts.
Clinical Significance:
- This image demonstrates not only acute pulmonary embolism but also its complication – pulmonary infarction.
- Pulmonary infarction occurs due to: Prolonged vascular occlusion, impaired bronchial arterial compensation
- Patients with infarction may present with: Pleuritic chest pain, hemoptysis
Diagnostic Contribution:
This figure is important because it:
- Confirms the functional impact of embolism on lung tissue
- Differentiates simple embolism from complicated PE with infarction
- Helps explain clinical symptoms and severity
Radiology Insight (Expert Level):
- Pulmonary infarcts typically appear as: Peripheral wedge – shaped opacities, base abutting the pleura
- This corresponds to the classic: Hampton’s hump (on radiograph/CT)
- Sagittal views are particularly helpful for: Evaluating craniocaudal extent, Identifying posterior and basal lesions
Chest X – ray Findings
Although often normal:
Possible findings include:
- Hampton’s hump
- Westermark sign
- Pleural effusion
However, X – rays lack sensitivity and are mainly used to exclude other conditions.
Differential Diagnosis
Accurate radiology interpretation is essential to distinguish PE from:
Diagnosis Workflow in Emergency Settings
Step – by – Step Approach
- Clinical assessment (Wells score)
- D – dimer testing
- CT pulmonary angiography
- Ultrasound of upper extremity veins
- Cardiac evaluation (echo if unstable)
Role of Medical Imaging AI
Modern medical imaging AI enhances:
- Automated clot detection
- Risk stratification
- Workflow prioritization
AI tools can flag CT scan diagnosis abnormalities within seconds, improving survival in emergency settings.
Treatment Strategies
Initial Management
- Oxygen therapy
- Hemodynamic stabilization
Pharmacologic Treatment
- Anticoagulation (heparin, DOACs)
- Thrombolysis (in severe cases)
Interventional Options
- Catheter – directed thrombolysis
- Mechanical thrombectomy
Addressing Subclavian Thrombosis
- Remove the causative catheter
- Consider thoracic outlet decompression
Prognosis
Outcome depends on:
- Clot burden
- Right ventricular function
- Time to diagnosis
Mortality Rates
- Untreated PE: up to 30%
- Treated PE: <5–10%
Early CT scan diagnosis dramatically improves outcomes.
Key Takeaways
- Subclavian venous thrombosis is an underrecognized source of pulmonary embolism
- CT pulmonary angiography is essential for diagnosis
- Radiology interpretation must include evaluation of the upper extremity veins
- Medical imaging AI is transforming emergency diagnosis workflows
- Early detection saves lives
Quiz
Question 1. What is the most common CT finding in acute pulmonary embolism?
A. Lung consolidation
B. Pleural effusion
C. Cavitation
D. Bronchial thickening
E. Intraluminal filling defect
Correct Answer: E.
Explanation: The hallmark of PE on CT is a filling defect within contrast – enhanced pulmonary arteries.
Question 2. Which condition is most associated with subclavian vein thrombosis?
A. Hypertension
B. Diabetes
C. Repetitive arm motion
D. Asthma
E. Hyperthyroidism
Correct Answer: C.
Explanation: Effort thrombosis (Paget – Schroetter syndrome) is linked to repetitive upper limb activity.
Question 3. What CT finding suggests severe pulmonary embolism?
A. Small peripheral clot
B. Normal right ventricle
C. RV/LV ratio > 1
D. Clear lung fields
E. Mild pleural effusion
Correct Answer: C.
Explanation: Right ventricular dilation indicates hemodynamic compromise and severe PE.
FAQ Section
What is the best imaging test for pulmonary embolism?
CT pulmonary angiography is the gold standard for CT scan diagnosis of PE.
Can upper extremity thrombosis cause pulmonary embolism?
Yes. Subclavian vein thrombosis can embolize to the lungs and cause PE.
How accurate is medical imaging AI in detecting PE?
AI systems now achieve high sensitivity and specificity, helping radiologists make faster diagnoses.
Is pulmonary embolism visible on chest X – ray?
Usually not. X – rays are often normal and cannot reliably detect PE.
Recommended Reading
1. Title: Diagnosis of pulmonary embolism with spiral CT: comparison with pulmonary angiography and scintigraphy
Authors: M Remy-Jardin, J Remy, F Deschildre, D Artaud, J P Beregi, C Hossein-Foucher, X Marchandise, A Duhamel
Read the Full Article on Radiology

2. Title: The epidemiology of venous thromboembolism
Authors: John A Heit, Frederick A Spencer, Richard H White
Read the Full Article on Journal of Thrombosis and Thrombolysis

3. Title: Upper extremity deep vein thrombosis
Authors: P Prandoni, E Bernardi
Read the Full Article on Current Opinion in Pulmonary Medicine

4. Title: Pulmonary Embolism
Author: Samuel Z. Goldhaber
Read the Full Article on NEJM

Stay updated on all scientific advances on Hemostasis Today.
-
Jul 17, 2026, 04:28Redefining Thromboprophylaxis in Multiple Myeloma: Early VTE Emerges as the Critical Therapeutic Challenge
-
Jul 16, 2026, 20:25Ilham Benzidia: Leaving ISTH 2026 With New Ideas and New Collaborations
-
Jul 16, 2026, 20:23Eman Hassan: A Fantastic Platelets and Megakaryocytes Session at ISTH 2026
-
Jul 16, 2026, 20:22Sankara Nelson Noah II: Investigating the Temporal Dynamics of Platelet – Leukocyte Interactions in Early Sepsis
-
Jul 16, 2026, 20:20Joseph Pierre Aboumsallem: Paris Certainly Delivered This Week, and Not Just Because of the Heat
-
Jul 16, 2026, 19:53Louise St. Germain Bannon: The End of Congress, the Beginning of New Collaborations
-
Jul 16, 2026, 19:18Steve Humphreys: Learning From the Leading Experts at ISTH 2026
-
Jul 16, 2026, 19:02Kellie Machlus: Where Science Meets Friendship at ISTH 2026
-
Jul 16, 2026, 18:51Aaron Paul Kithcart: When Clinical Research Comes Together at ISTH 2026