

Priyansh Shah and Romit Bhattacharya Address Patients’ Concerns on GLP-1
Priyansh Shah, Internal Medicine Resident Albert Einstein College of Medicine, Founder and President at World Youth Heart Federation, shared on LinkedIn:
”Patients often say: ‘GLP-1s feel too new, what about long-term safety?’
This hesitation is common.
But the science behind GLP-1 receptor agonists is anything but new.
New American Journal of Preventive Cardiology article ‘Addressing patient concerns about the ‘newness’ and long-term safety of GLP-1 receptor agonists: A clinician’s guide to counseling’ with Romit Bhattacharya shows how clinicians can reframe this conversation
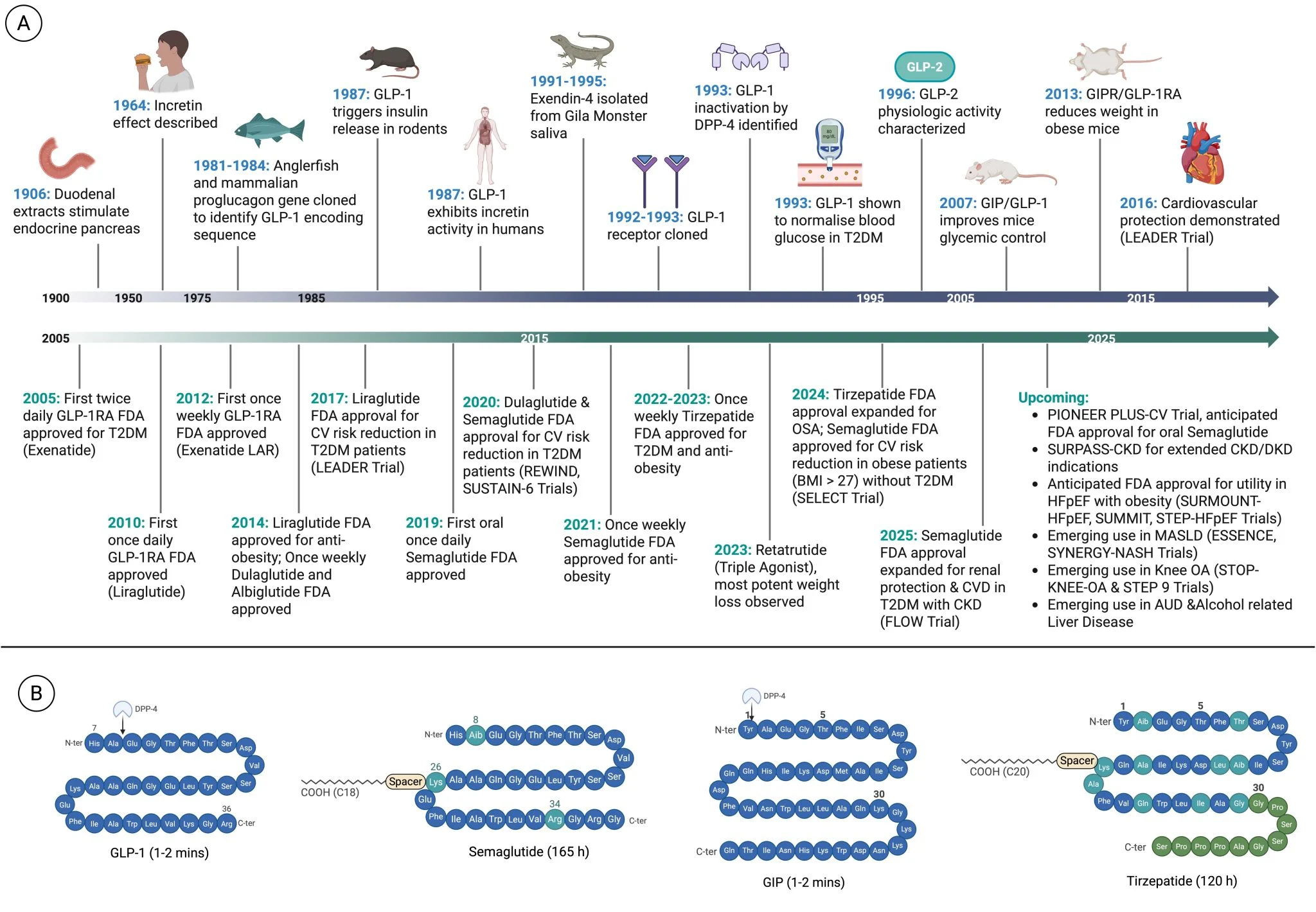
GLP-1 isn’t a trend, it’s decades old
- Incretin concept: early 1900s
- GLP-1 identified: 1980s
- First GLP-1RA approved: 2005
What feels ‘new’ to patients is actually the product of ~40+ years of research.
These drugs mimic a natural hormone
GLP-1RAs are ~98-99% identical to the GLP-1 your gut releases after meals.
Modern agents (semaglutide, tirzepatide) last longer, not act differently.
This matters for safety.
These aren’t just glucose-lowering drugs
GLP-1RAs show benefits across:
- CV outcomes (SELECT, SUSTAIN-6)
- Kidney disease (FLOW)
- HFpEF (STEP-HFpEF, SUMMIT)
- MASLD/MASH (emerging data)
They’re cardiometabolic therapies.
What about long-term data?
- 70,000 patients in major trials
- Millions treated worldwide
- ~20 years of pharmacovigilance
If major safety signals were there, we’d likely have seen them by now.
Side effects, set expectations early
Most common: nausea, vomiting, diarrhea
- Dose-dependent
- Usually transient
- Improved with slow titration + counseling
- Reassurance plus coaching go a long way.
Feared risks vs evidence
- Pancreatitis → not increased in large analyses
- Pancreatic cancer → no signal in long-term data
- Thyroid cancer → rodent-only MTC signal; not seen in humans
Context matters more than headlines.
Practical counseling checklist
- Explain physiologic mechanism
- Reiterate ~20 year track record
- Normalize GI effects
- Discuss rare risks when relevant
- Review logistics plus follow-up
Shared decisions are better than persuasion.
Bottom line
- GLP-1RAs aren’t experimental shortcuts.
- They’re mature, mechanism-based therapies backed by decades of science and real-world use.
When patients understand this, hesitancy often softens into informed choice.”
Romit Bhattacharya, Associate Director of the Cardiac Lifestyle Program at Massachusetts General Hospital, shared this post on LinkedIn, adding:
”Great Tweetorial from talented resident Priyansh Shah on our recent work published in American Journal of Preventive Cardiology!
GLP counseling in the clinic – how do we contextualize newer medical innovations in the context of their past scientific discoveries and clinical experience?
Check out the article and figures below.
Thanks to Khurram Nasir and Michael Shapiro for their highlighting of this work!”
Title: Addressing patient concerns about the ‘newness’ and long-term safety of GLP-1 receptor agonists: A clinician’s guide to counseling
Authors: Priyansh Shah, Romit Bhattacharya
Read the Full Article on American Journal of Preventive Cardiology

Stay updated on all scientific advances with Hemostasis Today.
{kind=link}
{kind=link}
-
Jun 29, 2026, 15:50Sweta Agrawal: Expanding Care for PNH Patients in Nepal
-
Jun 29, 2026, 15:17Heghine Khachatryan: Hemostasis at the Crossroads of Thrombosis and Bleeding
-
Jun 29, 2026, 15:07Tomaz Crochemore: From Bleeding to Thrombosis – The Era of Precision Hemostatic Medicine Has Arrived
-
Jun 29, 2026, 14:51Pete Stibbs: Building a Successful Venous Thrombectomy Practice
-
Jun 29, 2026, 14:30Bruno Pougault: Pregnancy and Thrombosis – Balancing Evolutionary Protection Against Clinical Risk
-
Jun 29, 2026, 13:32Omid Seidizadeh: The Full VWD Session from EHA 2026 Is Now Available to Watch
-
Jun 29, 2026, 13:22Cheryl Carcel: Make The Stroke Research More Inclusive for Women, Take The Survey
-
Jun 29, 2026, 13:18Bianca Rocca: New Expert Opinion On the Evolving Debate on Factor XI as a Therapeutic Target
-
Jun 29, 2026, 13:06Francisco Chacón-Lozsán: Intermittent Hemodialysis in the ICU Should not be Monitored Only by ‘Session Completed’