
AI Generated
Apr 12, 2026, 12:56
Chokri Ben Lamine: Clinical Dosing and Special Populations Guide for Apixaban
Chokri Ben Lamine, Adult Hematology and SCT Assistant Consultant at Oncology Center of Excellence at King Faisal Specialist Hospital and Research Center, shared a post on X:
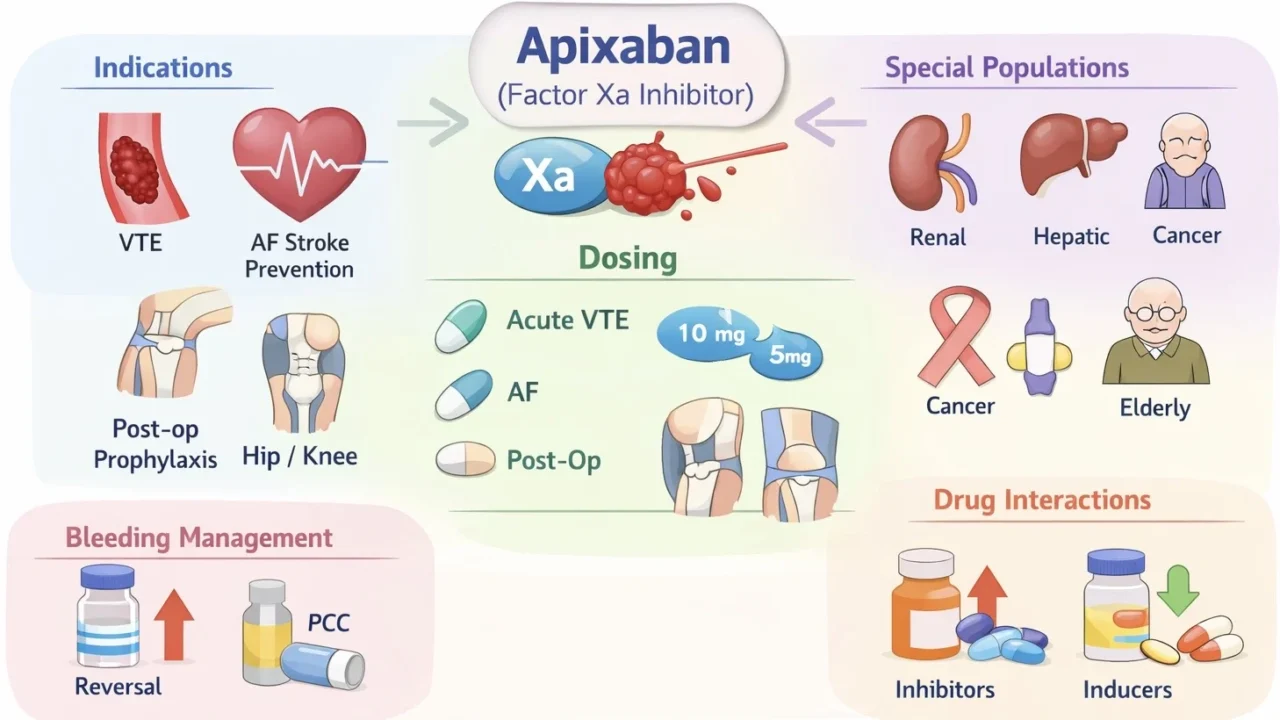
“Apixaban Pearls (Indications, Dosing plus, and Special Populations)
Mechanism
- Leads to Direct Factor Xa inhibitor leads to decrease thrombin generation
Indications
- VTE treatment (DVT/PE)
- Extended VTE prophylaxis
- Stroke prevention in AF (NVAF)
- Post-op prophylaxis (hip/knee)
Dosing (Adults)
Acute VTE
- 10 mg twice daily for 7 days
- Then 5 mg twice daily
Extended VTE
- 2.5 mg twice daily after at least 6 months of treatment
AF stroke prevention
- 5 mg twice daily
Dose reduction AF
- 2.5 mg twice daily if ≥2 of the following are present:
- Age ≥80 years
- Body weight ≤60 kg
- Serum creatinine ≥133 µmol/L (≈1.5 mg/dL)
Post-operative prophylaxis
- Hip replacement: 2.5 mg twice daily for 35 days
- Knee replacement: 2.5 mg twice daily for 12 days
Special Populations
Renal impairment
- Creatinine clearance ≥30 mL/min: standard dosing
- Creatinine clearance 15–29 mL/min: use with caution (dose reduction in atrial fibrillation)
- Creatinine clearance <15 mL/min or dialysis: limited evidence; avoid use (prefer warfarin)
Hepatic disease
- Mild (Child–Pugh A): use without dose adjustment
- Moderate (Child–Pugh B): use with caution
- Severe (Child–Pugh C): not recommended / contraindicated
Cancer-associated VTE
- Preferred option: DOAC in many patients (vs LMWH, depending on bleeding risk and cancer type)
- Avoid: if active gastrointestinal or genitourinary lesions due to increased bleeding risk
Obesity
- BMI >40 kg/m² or weight >120 kg: use with caution
- Consider drug level monitoring (anti–Xa activity) or alternative anticoagulation (LMWH or warfarin)
Elderly
- Increased bleeding risk
- Assess carefully for dose reduction criteria and comorbidities
Pregnancy
- Not recommended
- Use low-molecular-weight heparin (LMWH)
Breastfeeding
- Not recommended (insufficient safety data)
Antiphospholipid syndrome (APS)
- Not recommended, particularly in triple-positive APS
- Prefer warfarin
Drug interactions
- Strong CYP3A4/P-gp inhibitors (e.g., azoles, clarithromycin): increased bleeding risk
- Strong inducers (e.g., rifampin, carbamazepine): reduced efficacy
Bleeding management
- Specific reversal agent: andexanet alfa (if available)
- If unavailable: prothrombin complex concentrate (PCC)
Key pearl
- Apixaban has one of the safest bleeding profiles among direct oral anticoagulants in many hematology patients.”
Find more posts featuring Chokri Ben Lamine on Hemostasis Today.
-
Jul 12, 2026, 06:12Precision in Antithrombotic Therapy at ISTH 2026 – The Lancet Haematology
-
Jul 11, 2026, 23:36Emmanuel J Favaloro: A Fresh Perspective on the Manual Tilt Tube Method for PT and INR Determination
-
Jul 11, 2026, 21:44Timos Papagatsias: From Promising Concepts to Clinical Differentiation at ISTH 2026
-
Jul 11, 2026, 21:43Sharing New Research in Hemophilia at ISTH 2026 – Novo Nordisk Medical US
-
Jul 11, 2026, 21:41Bianca Constantin: Don’t Miss the ISTH Early Career Committee Activities
-
Jul 11, 2026, 21:38Fateme Babaha: Don’t Miss Your Favorite ISTH 2026 Sessions
-
Jul 11, 2026, 21:11Farjah Algahtani: Learning, Sharing, and Collaborating at ISTH 2026
-
Jul 11, 2026, 19:56Louise St. Germain Bannon: A Fantastic Start to ISTH 2026 and the Future of Thrombosis Research
-
Jul 11, 2026, 19:38Lynn Kloeckner: Recognizing Kirsten Lacine’s Impact on the Stroke Survivor Journey