
Chokri Ben Lamine: IV Iron Showdown – FCM vs Ferric Derisomaltose vs Iron Dextran
Chokri Ben Lamine, Assistant consultant at King Faisal Specialist Hospital and Research Center, shared a post on X:
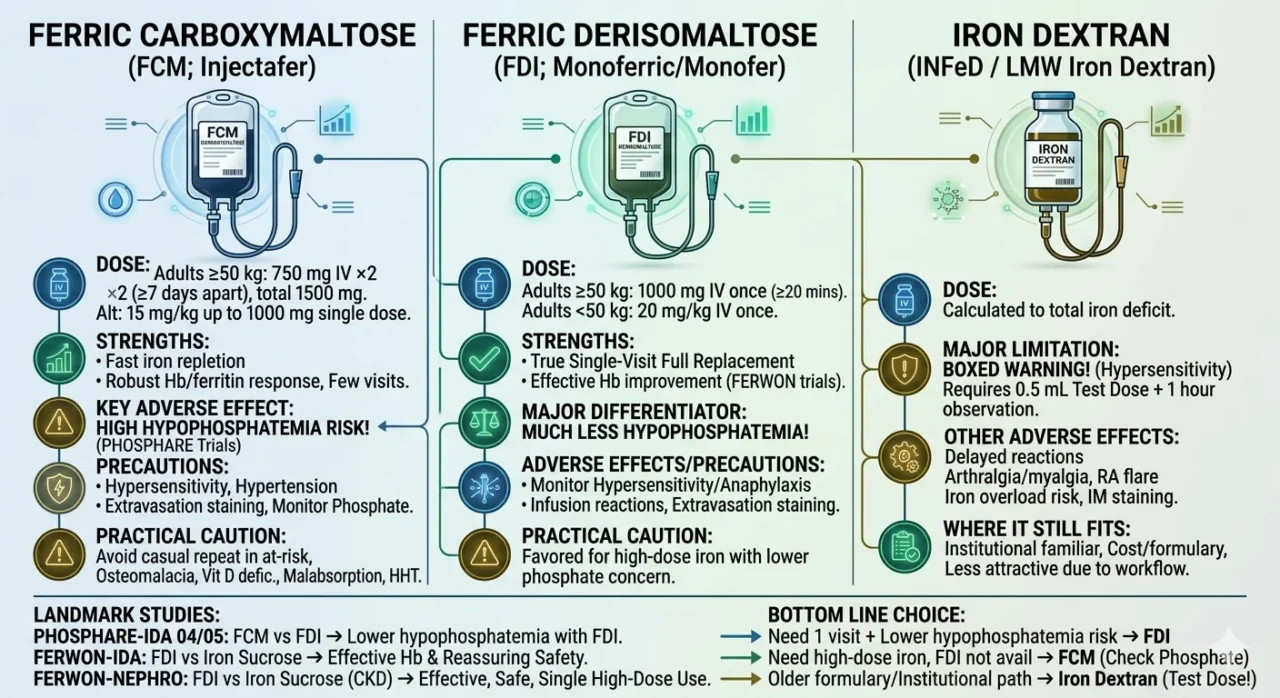
“IV iron showdown – FCM vs ferric derisomaltose vs iron dextran
Ferric carboxymaltose (FCM; Injectafer)
- Dose
Adults more than or equal to 50 kg: 750 mg IV ×2 doses at least 7 days apart, total 1500 mg/course; alternative 15 mg/kg up to 1000 mg as a single dose in some adults.
- Strengths and outcomes
Fast iron repletion, robust Hb/ferritin response, widely used when you want high-dose replacement with few visits.
Comparative data support efficacy similar to other modern IV irons.
- Key adverse effect
Biggest issue is hypophosphatemia. In the PHOSPHARE trials, hypophosphatemia was far more common with FCM than with ferric derisomaltose.
- Other precautions
Watch for hypersensitivity, hypertension, extravasation skin staining, and monitor phosphate in at-risk patients or before repeat courses.
Correct pre-existing hypophosphatemia first.
- Practical caution
Avoid casual repeat use in patients with prior FCM-related hypophosphatemia, osteomalacia risk, vitamin D deficiency, malabsorption, HHT, or other phosphate-wasting settings.
Ferric derisomaltose (FDI; Monoferric/Monofer)
- Dose
Adults more than or equal to 50 kg: 1000 mg IV once over at least 20 minutes.
Adults less than 50 kg: 20 mg/kg IV once. Repeat if IDA recurs.
- Strengths and outcomes
Excellent option when you want true single-visit full replacement.
In FERWON-IDA and FERWON-NEPHRO, it showed effective Hb improvement with low rates of serious/severe hypersensitivity, and the pooled safety analysis supported a favorable safety profile.
- Major differentiator
Compared with FCM, FDI causes much less hypophosphatemia.
This is the cleanest evidence-based reason many clinicians prefer it when available.
- Adverse effects and precautions
Still monitor for hypersensitivity/anaphylaxis, infusion reactions, and extravasation with possible long-lasting brown discoloration. Give only where resuscitation capability exists.
- Practical caution
Not ‘zero-risk’ for reactions, but in current practice it is often favored when you want high-dose iron with lower phosphate toxicity concern.
Iron dextran (INFeD / low-molecular-weight iron dextran)
- Dose
Dose is calculated to total iron deficit; the label allows incremental dosing until the calculated total is reached.
- Major limitation
This is the legacy product with boxed-warning hypersensitivity concern.
The U.S. label requires a 0.5 mL test dose before the first therapeutic dose and observation for at least 1 hour before giving the remainder of the first dose. Fatal reactions have occurred even after a tolerated test dose.
- Other adverse effects
Delayed reactions, arthralgia/myalgia, possible flare in rheumatoid arthritis, iron overload risk if diagnosis is wrong, and IM staining issues if given intramuscularly.
- Where it still fits
Useful when institutions are familiar with it or cost/formulary drives use, but from a modern practical standpoint it is usually less attractive than FCM/FDI because of the boxed warning and test-dose workflow.
Bottom line choice
- Need 1 visit and lower hypophosphatemia risk leads to Ferric derisomaltose
- Need effective high-dose iron and FDI not available leads to FCM, but think hard about phosphate
- Using an older formulary option / specific institutional pathway: iron dextran, but respect the boxed warning added test dose added observation
Landmark studies
- Phosphare-ida 04 / phosphare-ida 05: ferric derisomaltose vs ferric carboxymaltose: much lower hypophosphatemia with derisomaltose.
- Ferwon-ida: ferric derisomaltose vs iron sucrose in IDA: effective Hb response and reassuring safety.
- Ferwon-nephro: ferric derisomaltose vs iron sucrose in non-dialysis CKD with IDA: effective and safe, supports single high-dose use.
For iron dextran, modern practice is influenced more by current boxed-warning labeling and older comparative literature than by recent landmark superiority trials.”
Stay updated with Hemostasis Today.
-
Aug 3, 2026, 03:18Ajay Samkaria: Every Unexpected Antibody Tells a Story
-
Aug 3, 2026, 03:06Abdul Mannan: The Most Important Tube in the FXIII Assay
-
Aug 3, 2026, 02:29Herman Sandeep Prakasam: Who Is Missing Anticoagulation?
-
Aug 2, 2026, 23:07Akshat Jain: Redefining Hemophilia Readiness in Mexico
-
Aug 2, 2026, 16:24Satish Medakkar: The Importance of Early Recognition in Atypical Hemolytic Uremic Syndrome
-
Aug 2, 2026, 16:07Mirjavad Mammadov: Understanding the Thrombotic Paradox of Heparin Therapy
-
Aug 2, 2026, 15:49Munira Borhany: Advancing Equity in Women’s Hematological Care
-
Aug 2, 2026, 14:54Every Second Counts: How CPR and AEDs Can Save a Life – American Heart Association
-
Aug 2, 2026, 14:38New French Guidelines for Acquired Hemophilia A – CRH French Reference Center for Hemophilia Lyon