

Salvatore Massimo Petrina: When is it Truly Safe to Stop Anticoagulation after AF Ablation?
Salvatore Massimo Petrina, Hospital Physician in Cardiology at the Provincial Health Authority of Ragusa, shared a post on LinkedIn about a recent article by Tomoya Iwawaki at al., published in JACC: Clinical Electrophysiology, adding:
“When is it truly safe to stop anticoagulation after AF ablation?
A new study in JACC: Clinical Electrophysiology (Iwawaki et al., 2026) offers an unexpected answer: timing matters more than simple ‘procedural success.’
What they did
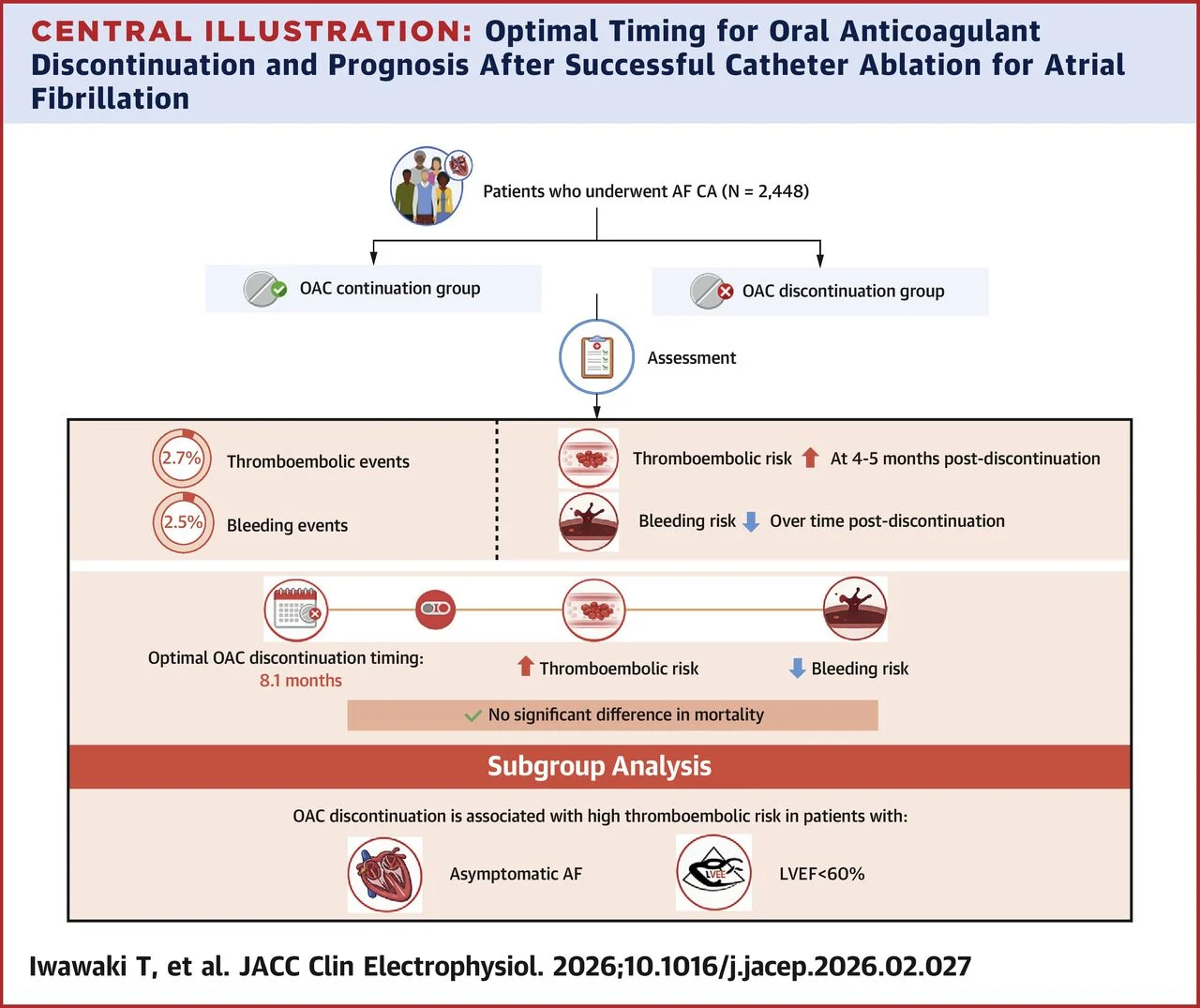
They retrospectively analyzed 2,448 post-catheter ablation AF patients, comparing those who discontinued OACs with those who continued, evaluating 537 time points (landmark analysis with IPTW).
The key finding
The ‘reverse net clinical benefit’ (balance between bleeding and thromboembolic risk) peaks at 8.1 months post-ablation.
Here is the risk curve:
- Months 4–5: peak thromboembolic risk after discontinuation
- Beyond 6 months: bleeding risk progressively declines
- Nearly 8 months: the optimal balance point
The numbers at the 8.1-month landmark:
- Thromboembolism HR: 2.36 (p=0.010) → the risk is real and measurable
- Major bleeding HR: 0.18 (p=0.002) → the bleeding benefit is real
- Mortality: no significant difference
But watch the subgroups
Discontinuation is particularly risky in:
- Patients with asymptomatic AF (silent recurrences!)
- Patients with LVEF <60%
My take-away
This study is not a license to stop all OACs at 8 months ‘by the calendar.’
It is an elegant signal telling us: the decision is dynamic, not binary.
The 8.1-month optimum is population-level data, not a protocol to apply to everyone.
CHA₂DS₂-VASc stratification, post-ablation rhythm monitoring, and individual clinical status (especially LVEF and symptoms) remain the main compass.
Reflection:
How many of us have a structured conversation with the patient at 3–6–12 months post-ablation to reassess anticoagulant therapy, rather than leaving it as a ‘legacy’ from discharge?
Disclaimer:
This post is for educational and scientific update purposes only.
It does not constitute medical advice, therapeutic recommendation, or a substitute for individual clinical judgment.
Decisions on post-ablation anticoagulation must be made on a case-by-case basis, in accordance with current guidelines (ESC/AHA/ACC/HRS) and the individual patient’s embolic/bleeding risk assessment.”
Title: Optimal Timing for Oral Anticoagulant Discontinuation and Prognosis After Successful Catheter Ablation for Atrial Fibrillation
Authors: Tomoya Iwawaki, Satoshi Yanagisawa, Yasuya Inden, Kiichi Miyamae, Hiroyuki Miyazawa, Takayuki Goto, Shun Kondo, Masaya Tachi, Taishi Fukushima, Takehiro Hiramatsu, Kentaro Adachi, Tsubasa Teraoka, Ryusuke Ota, Masafumi Shimojo, Yukiomi Tsuji, Takahiro Okumura, Toyoaki Murohara

Stay updated on all scientific advances with Hemostasis Today.
{kind=link}
-
Jun 29, 2026, 12:44Sumedha Dash: Inspiring the Next Generation of Voluntary Blood Donors at CV Raman Global University
-
Jun 29, 2026, 12:35Dilini Christina Ranasinghe: Behind Every Unit of Blood
-
Jun 29, 2026, 06:48Christina Pohlman: Anticoagulants and Bone Health – APS Awareness Month Day 23
-
Jun 29, 2026, 06:33Andreas Calatzis: Can Fibrinolysis Sensitivity Be Claimed Without a Reference Standard
-
Jun 29, 2026, 06:25Aliaa Albadri: When a Hair Wash Leads to a Stroke Workup
-
Jun 29, 2026, 06:22Tehreen Parveen: Historical Milestone in Drug Discovery – The Discovery of Aspirin
-
Jun 29, 2026, 06:16Muhammad Sufyan: Deep Vein Thrombosis – Recognizing the Warning Signs
-
Jun 29, 2026, 05:33Janak Sadhu: Uniting for The Stroke-Free Mehsana Initiative
-
Jun 29, 2026, 05:20Deepti Sachan: A Global Exchange Shaping the Future of Transfusion Medicine at ISBT 2026