
AI generated
Apr 2, 2026, 08:22
Chokri Ben Lamine: Laboratory Findings and Management of Severe Type 3 von Willebrand Disease
Chokri Ben Lamine, Adult Hematology and SCT Assistant Consultant at Oncology Center of Excellence at King Faisal Specialist Hospital and Research Center, shared a post on X:
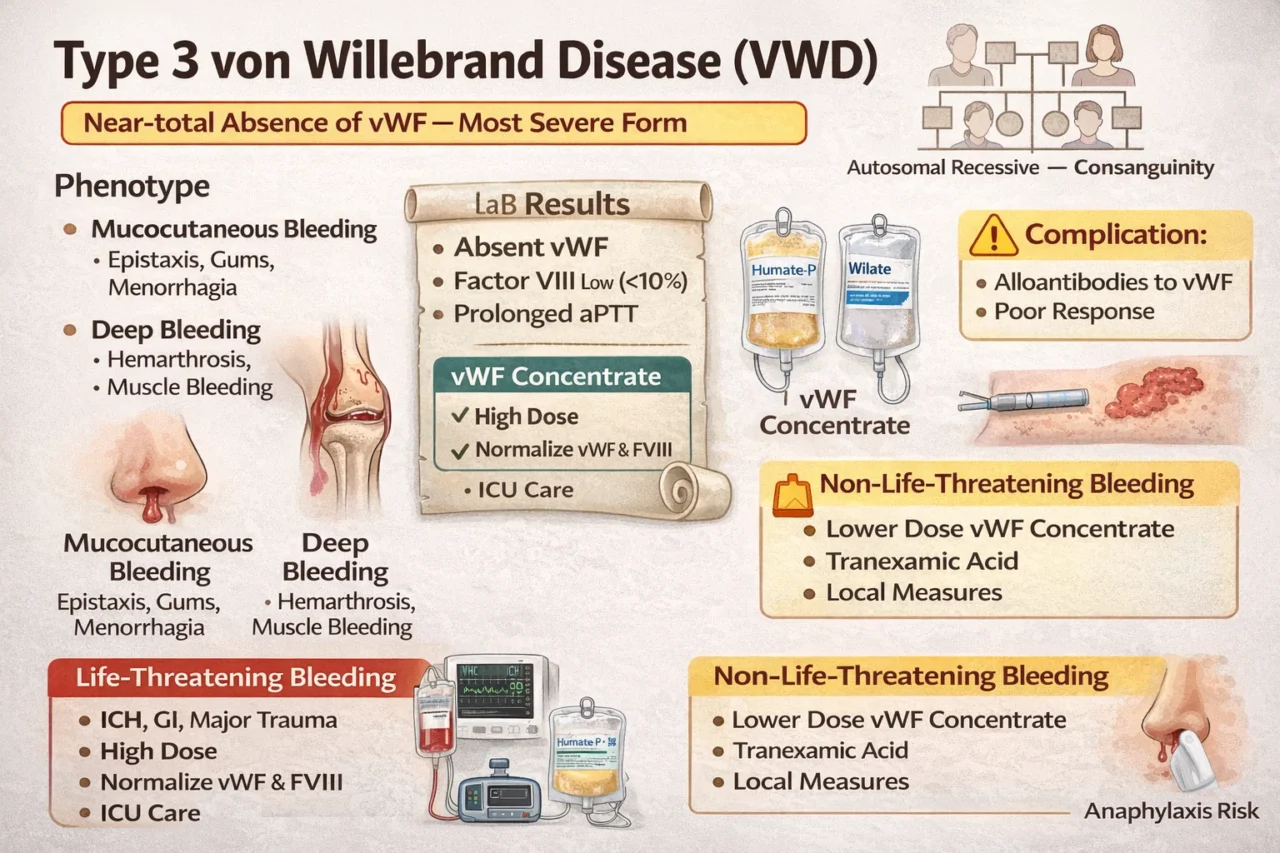
“Type 3 VWD equals near‑total absence of vWF, which is the most severe form.
Family – autosomal recessive; think consanguinity.
Phenotype
- Mucocutaneous bleeding (epistaxis, gums, menorrhagia)
- Deep bleeding, such as hemarthrosis and muscle bleeding, results in a clinical picture that mimics hemophilia A.
Labs
- vWF:Ag and activity absent
- Factor VIII very low – less than ten percent.
- aPTT prolonged
- PT normal
Pearl: DDAVP is ineffective because there is no endogenous von Willebrand factor available to release.
Life-threatening bleeding (ICH, GI, major trauma)
- Immediate vWF-containing concentrate (Humate-P, Wilate) high dose
- Target: normalize vWF activity and FVIII rapidly
- Repeat dosing q8-12h based on levels/clinical response
- Add FVIII if levels critically low or delayed response
- ICU-level care plus local hemostatic measures
Non–life-threatening bleeding (epistaxis, menorrhagia, minor procedures)
- vWF-containing concentrate (lower dose / shorter duration)
- Tranexamic acid for mucosal bleeding
- Local measures (pressure, topical TXA, nasal packing, etc.)
Complication: Alloantibodies to vWF lead poor response / anaphylaxis risk change symbols to words.”
Stay updated with Hemostasis Today.
-
Jul 13, 2026, 23:39Yaariv Khaykin: Whole-Person Care Can Strengthen Stroke Prevention in Patients With Atrial Fibrillation
-
Jul 13, 2026, 22:33ESOC 2026 recordings are now available on eSTEP – European Stroke Organisation
-
Jul 13, 2026, 20:17Julia R. Coleman: Fantastic First Day at ISTH 2026
-
Jul 13, 2026, 20:11Ruah Alyamany: Combination Therapy Improves Quality of Life in ITP
-
Jul 13, 2026, 19:47Brian O Mahony: Two-Year Results of BBM-H901 Gene Therapy Presented at ISTH 2026
-
Jul 13, 2026, 19:37Sara Zalghout: Connecting With Colleagues From All Over the World at ISTH 2026
-
Jul 13, 2026, 18:54Alfonso J. Tafur: New Evidence on Perioperative Anticoagulation in Cancer at ISTH 2026
-
Jul 13, 2026, 18:42Jessica Garcia: Thrombin Generation in Type 3 VWD With an Inhibitor on Emicizumab
-
Jul 13, 2026, 18:19Fionnuala Ní Áinle: High-Quality Evidence for DVT Diagnosis in Pregnancy at ISTH 2026