
AI Generated
Apr 30, 2026, 12:45
Chokri Ben Lamine: Methemoglobinemia in Hematology – Causes, Diagnosis, Antidote
Chokri Ben Lamine, Assistant consultant at King Faisal Specialist Hospital and Research Center, shared a post on X:
“Methemoglobinemia in Hematology – Causes, Dx, Antidote
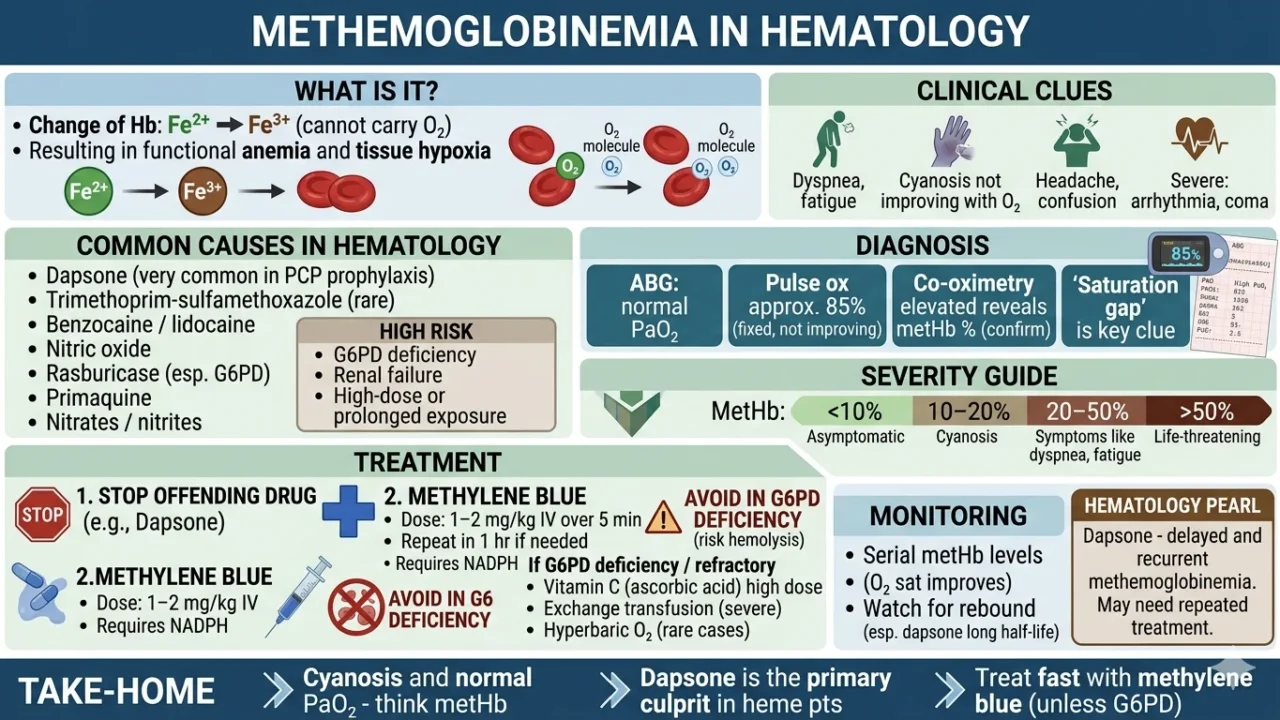
What is it?
Hb Fe²⁺ to Fe³⁺ leading to cannot carry O₂
Resulting in functional anemia and tissue hypoxia
Common causes in Hematology
- Dapsone (very common in PCP prophylaxis)
- Trimethoprim-sulfamethoxazole (rare)
- Benzocaine / lidocaine
- Nitric oxide
- Rasburicase (esp. G6PD)
- Primaquine
- Nitrates / nitrites
High risk:
- G6PD deficiency
- Renal failure
- High-dose or prolonged exposure
Clinical clues
- Dyspnea, fatigue
- Cyanosis not improving with O₂
- Headache, confusion
- Severe: arrhythmia, coma
Diagnosis
- ABG: normal PaO₂
- Pulse ox approximately 85% (fixed, not improving)
- Co-oximetry elevated reveals metHb % (confirm)
‘Saturation gap’ is key clue
Severity guide
- less than 10% – often asymptomatic
- 10–20% – cyanosis
- 20–50% – symptoms (dyspnea, fatigue)
- more than 50% – life-threatening
Treatment
1. STOP offending drug (e.g., Dapsone)
2.Methylene blue
- Dose: 1–2 mg/kg IV over 5 min
- Repeat in 1 hr if needed
Requires NADPH
- Avoid in G6PD deficiency (risk hemolysis)
If G6PD deficiency / refractory
- Vitamin C (ascorbic acid) high dose
- Exchange transfusion (severe)
- Hyperbaric O₂ (rare cases)
Monitoring
- Serial metHb levels
- Clinical response (O₂ sat improves)
- Watch for rebound (esp. dapsone long half-life)
Hematology pearl
- Dapsone – delayed and recurrent methemoglobinemia
- May need repeated treatment
Take-home
- Cyanosis and normal PaO₂ – think metHb
- Dapsone is the primary culprit in hematology patients
- Treat fast with methylene blue (unless G6PD).”
Other posts featuring Chokri Ben Lamine on Hemostasis Today.
-
Jun 24, 2026, 13:50Tijjani Balas: Why Early Detection of DVT Matters
-
Jun 24, 2026, 13:43Brandon Michael Henry: Interpreting Complement Activation After AAV Gene Therapy
-
Jun 24, 2026, 13:37Heba Youssef: Heparin-Induced Thrombocytopenia – The Prothrombotic Emergency You Cannot Miss
-
Jun 24, 2026, 13:32Jecko Thachil: Understanding the Clinical Spectrum of Vitamin B12
-
Jun 24, 2026, 13:32Namrata Singh: Beyond Low Platelets – Understanding What Triggers ITP
-
Jun 24, 2026, 09:29Advancing Women’s Health Through Collaboration with Jean Hailes for Women’s Health – Stroke Foundation
-
Jun 24, 2026, 09:18The Lasting Immunological Footprint of VITT – JTH
-
Jun 24, 2026, 09:09Umberto Pensato: Dedicated Funding Pathways for Stroke Research in Italy
-
Jun 24, 2026, 09:00Danny Gaskin: BBTS 2026 and the Evolving Role of Transfusion in Maternity Care