

Peter Antevy: When She’s Bleeding Out, The Blood Type in the Cooler Shouldn’t Decide Whether She Lives
Peter Antevy, Founder and Chief Medical Officer at Handtevy, shared a post on LinkedIn about a recent article by Matthew J. Levy published in Transfusion, adding:
“A 24-year-old woman is pinned in the driver’s seat of a rolled SUV on a rural highway.
Her pulse is thready.
Her systolic blood pressure is in the 70s.
The flight crew is 18 minutes out.
Your ground unit carries low-titer O-positive whole blood.
She’s bleeding to death.
You reach for the cooler.
And then someone asks the question that has paralyzed EMS systems across the country:
‘What if she’s RhD-negative?’
That question, asked at the wrong time, in the wrong way, has cost women their lives. Not because the concern isn’t valid. It is.
But because the answer has been so poorly understood that clinicians have defaulted to hesitation when the science says act.
A landmark paper just published in Transfusion finally puts the best practices in writing.
The Paper
The THOR Network Foundation (Trauma, Hemostasis, and Oxygenation Research) Network, in collaboration with The Allo Hope Foundation and supported by the U.S. Department of Defense, has published a comprehensive best-practices document for managing life-threatening hemorrhage in females of childbearing potential (FCP).
The paper, authored by leaders from Johns Hopkins, DC Fire and EMS, Harris County Emergency Services, the University of Pittsburgh, and several other institutions, was published in Transfusion in 2026.
This isn’t a theoretical exercise.
It’s an operational playbook.
The Problem We Created
Prehospital blood programs are expanding across the United States.
By 2024, over 300 trauma centers had incorporated low-titer O-positive whole blood (LTOWB) into clinical practice.
Roughly 60 to 75 percent of air medical transport systems now carry blood products, and a growing number of ground units are following.
Most of these programs carry O-positive products because O-negative supply is critically limited.
Only about 3 to 4 percent of the U.S. population can donate low-titer O-negative blood.
The math doesn’t work. The demand far exceeds the supply.
Here is where the tension lives.
When an RhD-negative woman of childbearing potential receives RhD-positive blood, there is a risk of alloimmunization.
Her immune system can develop antibodies against the RhD antigen, and those antibodies can cross the placenta in a future pregnancy and attack fetal red blood cells.
The result is hemolytic disease of the fetus and newborn, or HDFN.
HDFN ranges from mild jaundice to severe fetal anemia, hydrops, and death.
That is a real risk.
But here is what the fear-based narrative gets wrong: the probability of that outcome is far lower than most clinicians believe, and the systems we now have to manage it are far better than most clinicians realize.
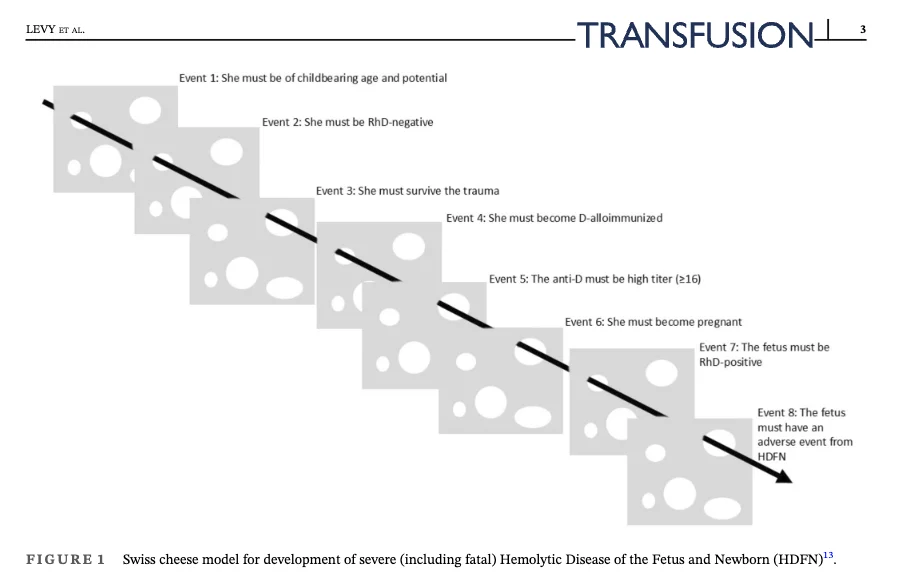
The Math That Should Change the Conversation
The paper presents a Swiss cheese model illustrating the sequential events that must all occur for a case of severe HDFN to develop.
The patient must be of childbearing age and potential.
She must be RhD-negative.
She must survive the trauma.
She must become D-alloimmunized.
The anti-D must reach high titer.
She must become pregnant.
The fetus must be RhD-positive.
And even then, the fetus must develop a clinically significant adverse event from HDFN.
One model estimated one case of fetal death or permanent disability per 670 RhD-positive transfusions in RhD-negative FCP.
That is roughly 0.15 percent.
Another model estimated a 0.04 percent chance of perinatal death and a 0.24 percent chance of death or other serious adverse event.
Compare that to the near certainty of death from uncontrolled hemorrhagic shock without transfusion.
The risk-benefit calculation is not close.
The Equity Problem
Here is a finding from the paper that should make every EMS medical director uncomfortable: on adjusted analysis, females of childbearing potential were 40 percent less likely to receive LTOWB than males.
Forty percent.
That means women in hemorrhagic shock are being treated differently because of a theoretical future risk, while men with the same injury and the same physiology get the blood that could save them.
The paper makes the point clearly: withholding prehospital blood products from women, or defaulting to scarce RhD-negative red-cell-only transfusions while men receive LTOWB, intentionally widens survival gaps.
We would never accept a protocol that said ‘withhold defibrillation from women in cardiac arrest because it might affect a future pregnancy.’
Yet that is functionally what some systems are doing with blood.
What the Best Practices Say
The THOR Network’s guidance is clear, practical, and built for the field.
The key principles center on a few critical themes.
First, life-threatening hemorrhage takes priority.
The immediate risk of death from hemorrhagic shock outweighs the potential future risk of HDFN.
Do not delay transfusion when RhD-negative blood is unavailable.
Use RhD-positive LTOWB or RBCs to preserve life.
Second, communication is everything.
EMS must document and communicate every RhD-positive transfusion to the receiving hospital.
The handoff is a critical juncture.
Hospitals need to know what was given so blood banks can act.
The paper highlights the STRAC prehospital blood product transfusion record as an example of how to standardize this process.
Third, Rh immunoglobulin (RhIg) has a role, but a limited one.
RhIg is recommended only after small-volume exposure of one unit or less to RhD-positive products in RhD-negative FCP.
It is not recommended after large-volume resuscitation during exsanguinating hemorrhage.
When indicated, it can be given up to 72 hours after exposure.
There is no role for RhIg in males or postmenopausal females.
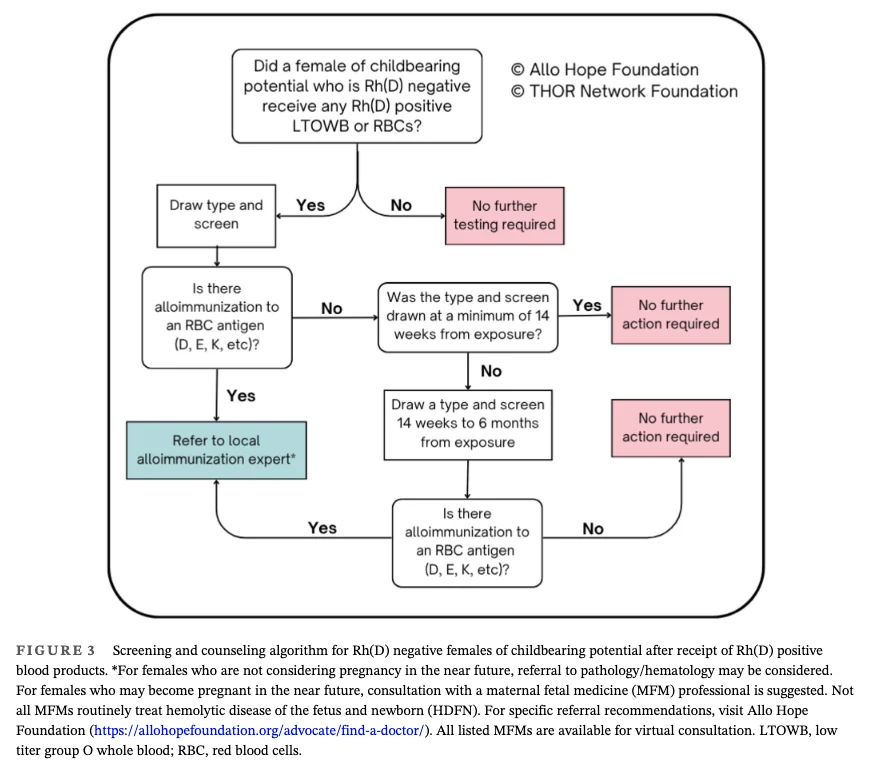
Fourth, follow-up and counseling are non-negotiable.
All RhD-negative FCP who receive RhD-positive blood products should receive standardized informational materials before discharge, including clear documentation of what was transfused and why.
Antibody screening should be scheduled between 14 weeks and 6 months post-exposure, and results should be shared with outpatient clinicians and maternal-fetal medicine specialists.
What This Means for Systems
This paper gives EMS and hospital leaders a framework to build around. It is not enough to carry blood on an ambulance or helicopter.
Systems need protocols that address the entire continuum: field recognition, rapid initiation of balanced resuscitation, EMS-to-hospital handoff, post-exposure testing, counseling, and long-term follow-up.
The paper also points toward future directions that matter.
Multicenter trials including MATIC-2 and TROOP are ongoing and will generate critical data on LTOWB outcomes, alloimmunization rates, and adverse events in both adult and pediatric populations.
Registries need to track the cumulative burden of alloimmunization and the proportion of patients who develop clinically significant high-titer antibodies.
Digital hemovigilance linking EMS records, hospital transfusion services, and regional blood banks can enable real-time detection, targeted counseling, and transparent reporting.
And on the horizon, the development of RBC antigen-agnostic blood products, including stem cell-derived and artificial red cells, could one day eliminate this dilemma entirely.
The Bottom Line
The science has caught up to the scenario every prehospital clinician has faced or will face.
A woman is hemorrhaging.
The blood on the shelf is O-positive.
The question is no longer whether to give it.
The question is whether your system is ready for what comes after.
Give the blood. Save her life. Document it. Communicate it. Follow up.
That is the standard.
And now we have the evidence-based framework to hold ourselves to it.”
Title: The THOR network best practices for females of childbearing potential with life-threatening hemorrhage: Guidance for emergency medical services and hospitals
Authors: Matthew J. Levy, Holly OByrne, Eric A. Bank, Jeremy W. Cannon, Andew P. Cap, Elon Glassberg, John B. Holcomb, Donald H. Jenkins, Christine Leeper, Molly R. Sherwood, Kevin R. Ward, Mark H. Yazer, Philip C. Spinella
Read the Full Article on Transfusion.

Stay updated with Hemostasis Today.
{kind=link}
{kind=link}
-
Jul 9, 2026, 11:54Deepak Pradhan։ Can Withaferin-A Help Combat Drug-Resistant Malaria?
-
Jul 9, 2026, 11:26Peter Zhang: Is Canada Ready for the Gene Therapy Era?
-
Jul 9, 2026, 09:35Pradeebha Muthukumar: Do You Know the Signs of Anemia?
-
Jul 9, 2026, 09:24Maryam Majid: Machine Learning for Anemia Risk Prediction
-
Jul 9, 2026, 08:46Jordan Agay: Folate Deficiency in Patients Receiving PARP Inhibitors
-
Jul 9, 2026, 08:29Laura Katz: Is Human Lactoferrin Better Than Bovine Lactoferrin?
-
Jul 9, 2026, 08:17Anziya Sabeer: AI-Driven Non-Invasive Anemia Detection
-
Jul 9, 2026, 07:37Variable Mechanisms of ADAMTS13 Inhibition by Autoantibodies in iTTP – JTH
-
Jul 9, 2026, 07:31DHR-Sponsored Training Programme at ICMR-CRMCH Week 2 – Day 4 – ICMR-NIRBID