

8 Posts Not to Miss From the ASH 2025 – Marc Carrier
The American Society of Hematology Congress 2025 (ASH25) is officially underway in Orlando, Florida, from December 6 to 9.
It aims to bring together hematology professionals from across the globe.
Throughout the meeting, experts presented new research, clinical breakthroughs, and innovations that are defining the future of hematologic care.
Marc Carrier, Professor at Ottawa Hospital Research Institute, shared following posts from ASH 2025 on LinkedIn and X:
1.”New Insights on Bleeding Risk During Extended Anticoagulation in Cancer-Associated VTE
Presented at ASH25 and published in Lancet Haematology, this post-hoc analysis of the API-CAT trial, led by Prof. Isabelle Mahé identifies key predictors of clinically relevant bleeding during extended apixaban therapy in patients with active cancer.
Key Predictors of Higher Bleeding Risk
• Anemia and/or thrombocytopenia (HR 1.93)
• Age ≥75 years (HR 1.51)
• Index pulmonary embolism (HR 1.47)
• Male sex (HR 1.38)
These predictors were consistent across cancer types and also aligned with predictors of major bleeding.
See manuscript.
 ”
”
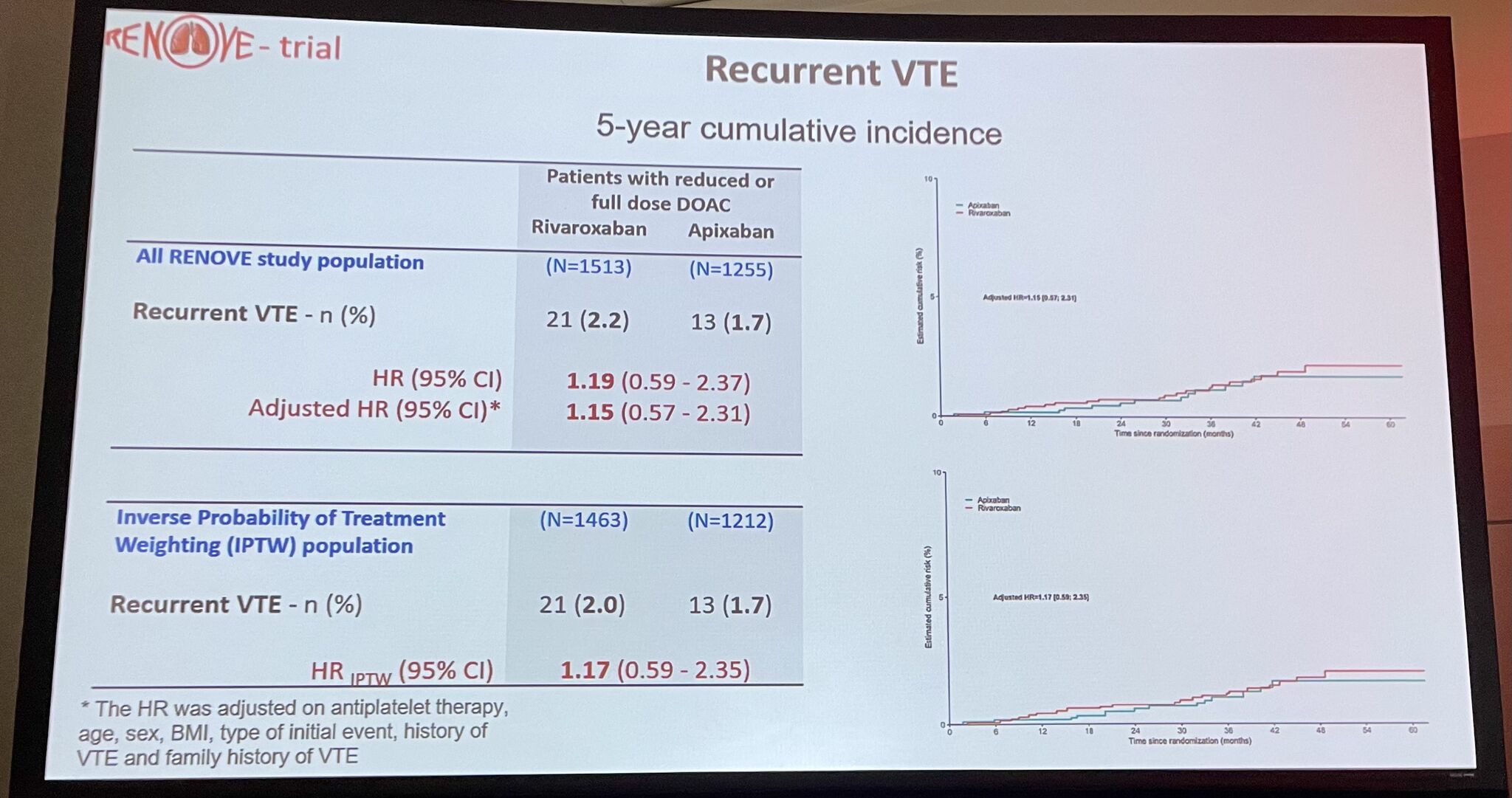
2.”ASH25 Highlight – Extended Anticoagulation in VTE: Apixaban vs Rivaroxaban
Important new insights from a post-hoc analysis of the RENOVE randomized trial, evaluating safety during extended treatment (after ≥6 months of full-dose therapy) with apixaban or rivaroxaban by Prof Francis Couturaud
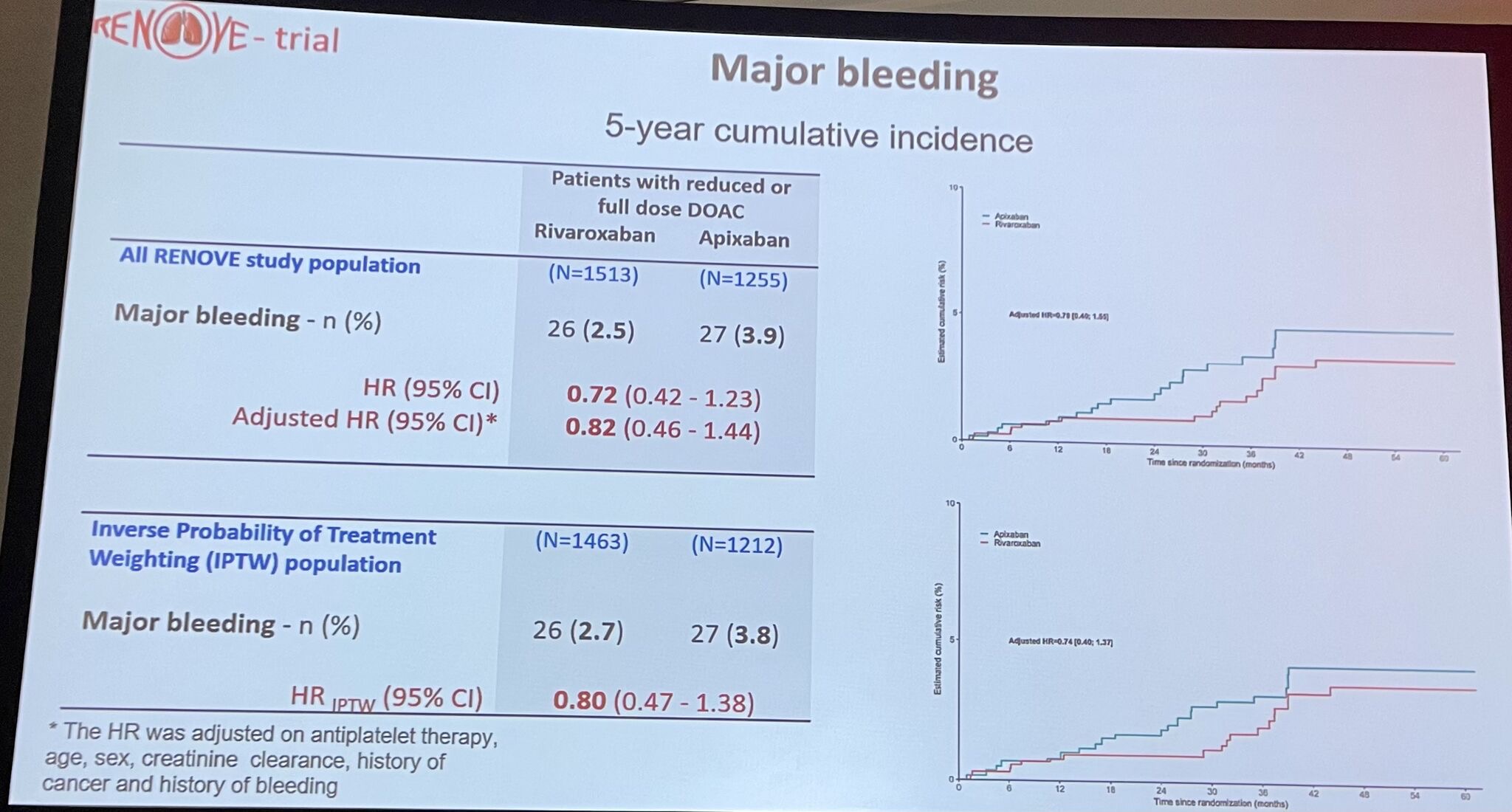
Key Findings (5-year outcomes):
• Clinically relevant bleeding (CRB): Similar between drugs at both full and reduced doses.
• Major bleeding: No significant differences across subgroups.
• Recurrent VTE: Low and comparable with both agents.
• Dose reduction: Consistently lowered CRB risk for both apixaban and rivaroxaban.
Takeaway:
Unlike early-treatment data where rivaroxaban shows higher bleeding risk, during extended therapy the safety profiles of apixaban and rivaroxaban appear equivalent.
More trials are needed.
Read the full article here.
 ”
”
3.”Congratulations to Dr. Mysa Saad on her first oral presentation at ASH25!
Does concurrent antiplatelet or NSAID use increase bleeding risk in cancer patients receiving apixaban thromboprophylaxis?
Key Findings:
• Among patients receiving prophylactic apixaban, concurrent antiplatelet/NSAID use significantly increased clinically relevant bleeding (HR 1.78) and CRNMB (HR 1.98).
• No reduction in VTE was observed (HR 0.60).
• In subgroup analyses:
– Antiplatelet agents were the main driver of increased bleeding (CRNMB HR 2.59).
– NSAIDs did not show a significant impact on bleeding or VTE.
• Mortality outcomes were unaffected.
Implications:
These results highlight the need to carefully reassess antiplatelet/NSAID indications and conduct individualized bleeding risk evaluations when considering apixaban prophylaxis in cancer outpatients.
Read the full article here.

 ”
”
4.”Huge congratulations to Dr. Abdulrahman Al Raizah on delivering his first ASH presentation!
His team’s quality-improvement project tackled two major challenges in IVC filter use: insertion without proper indication and delayed retrieval.
Through a coordinated, system-level strategy, they achieved:
• Appropriate filter use: 72.7% → 91.4%
• Retrieval among eligible patients: 76% → 92.3%
• Median retrieval time: reduced from 35 to 22 days
A fantastic example of how evidence-based policy, education, and workflow redesign can meaningfully improve thrombosis care.
Read the full article here.
 ”
”
5.”Congratulations to Dr. Elena Butera on her first poster presentation at ASH!
An important contribution to the limited evidence base on cancer-associated ovarian and renal vein thrombosis (OVT/RVT).
Study highlights (n = 82):
• 98% of OVT/RVT events were incidental
• 82% received anticoagulation (64% LMWH, 31% DOAC)
• Recurrent VTE: 3.8% at 6 and 12 months
↳ 1.5% with AC vs. 14.3% without
• Major bleeding: 2.5%, all on therapeutic LMWH
• 12-month mortality: 25%
Takeaway: Anticoagulation appears effective with modest bleeding risk, providing valuable real-world data for these rare and understudied unusual-site VTEs.
Read the full article here.”
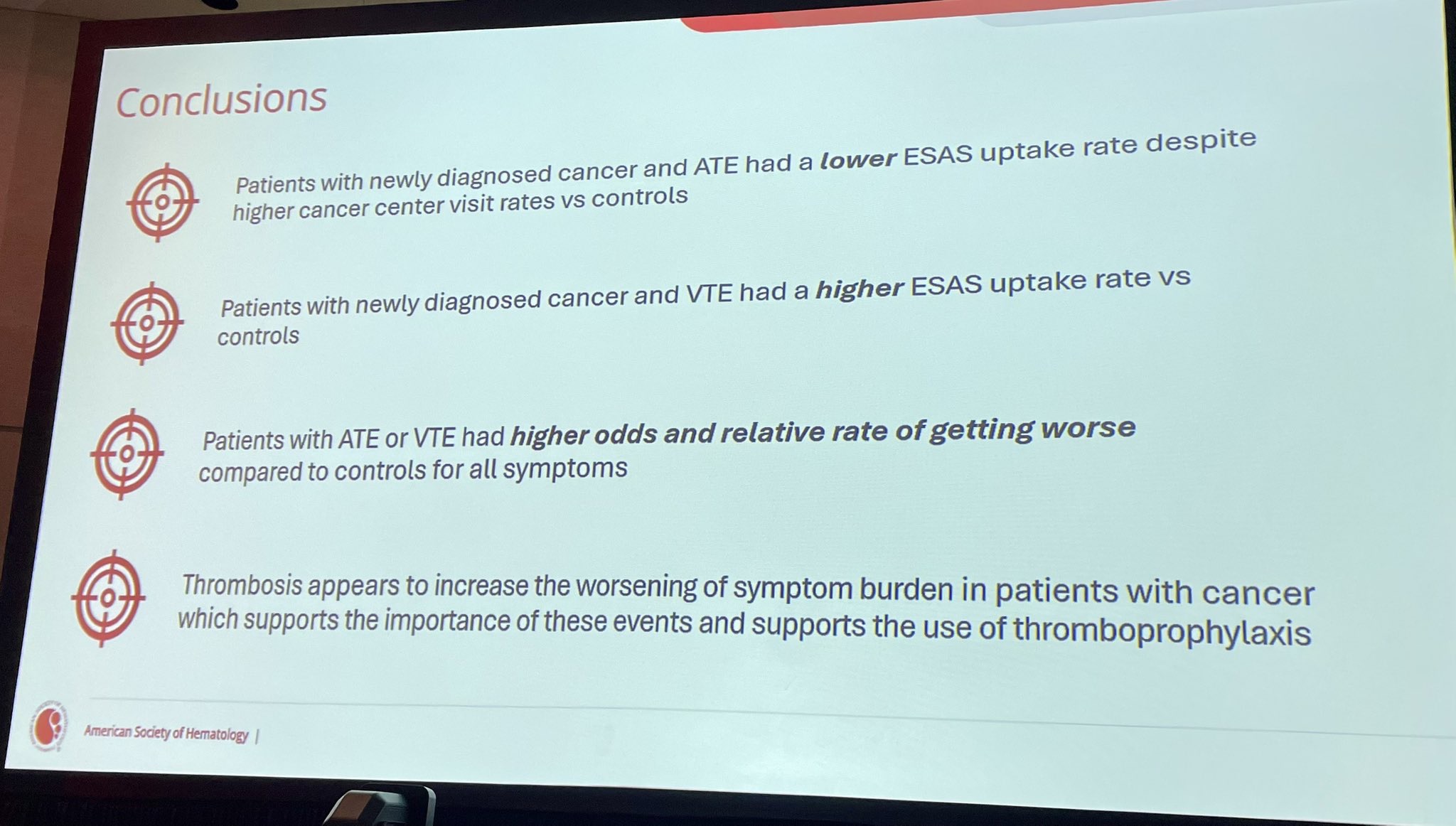
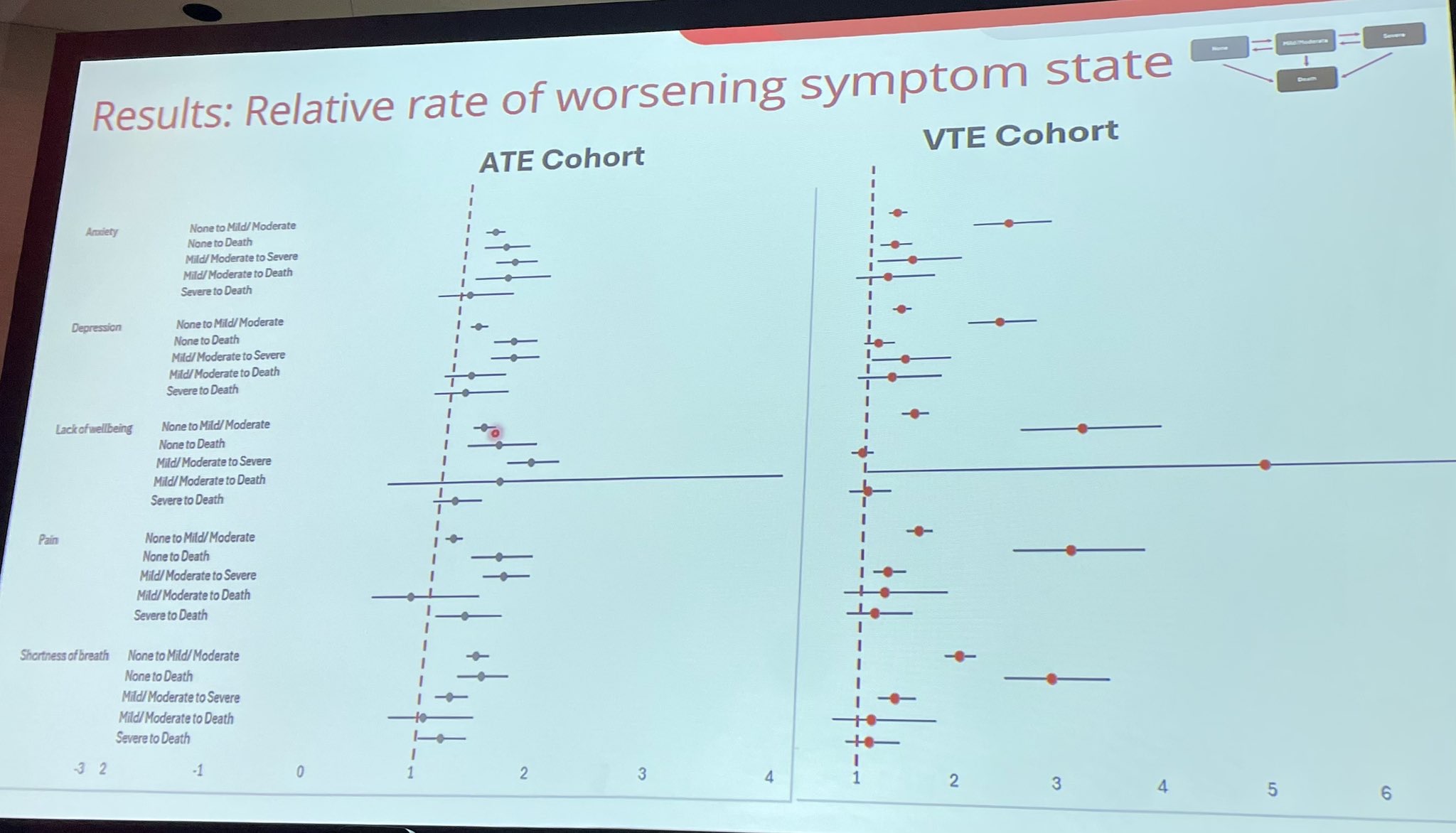
6.”ATE and VTE worsen symptom burden in cancer
In a population study (n≈59K), ATE lowers ESAS uptake, despite high clinic visits, while VTE increases ESAS use.
Both ATE and VTE led to higher odds of worsening pain, anxiety, depression, SOB and wellbeing.
Supports better monitoring + thromboprophylaxis.
Read the full article by Deborah Siegal and Colleagues here.
 ”
”
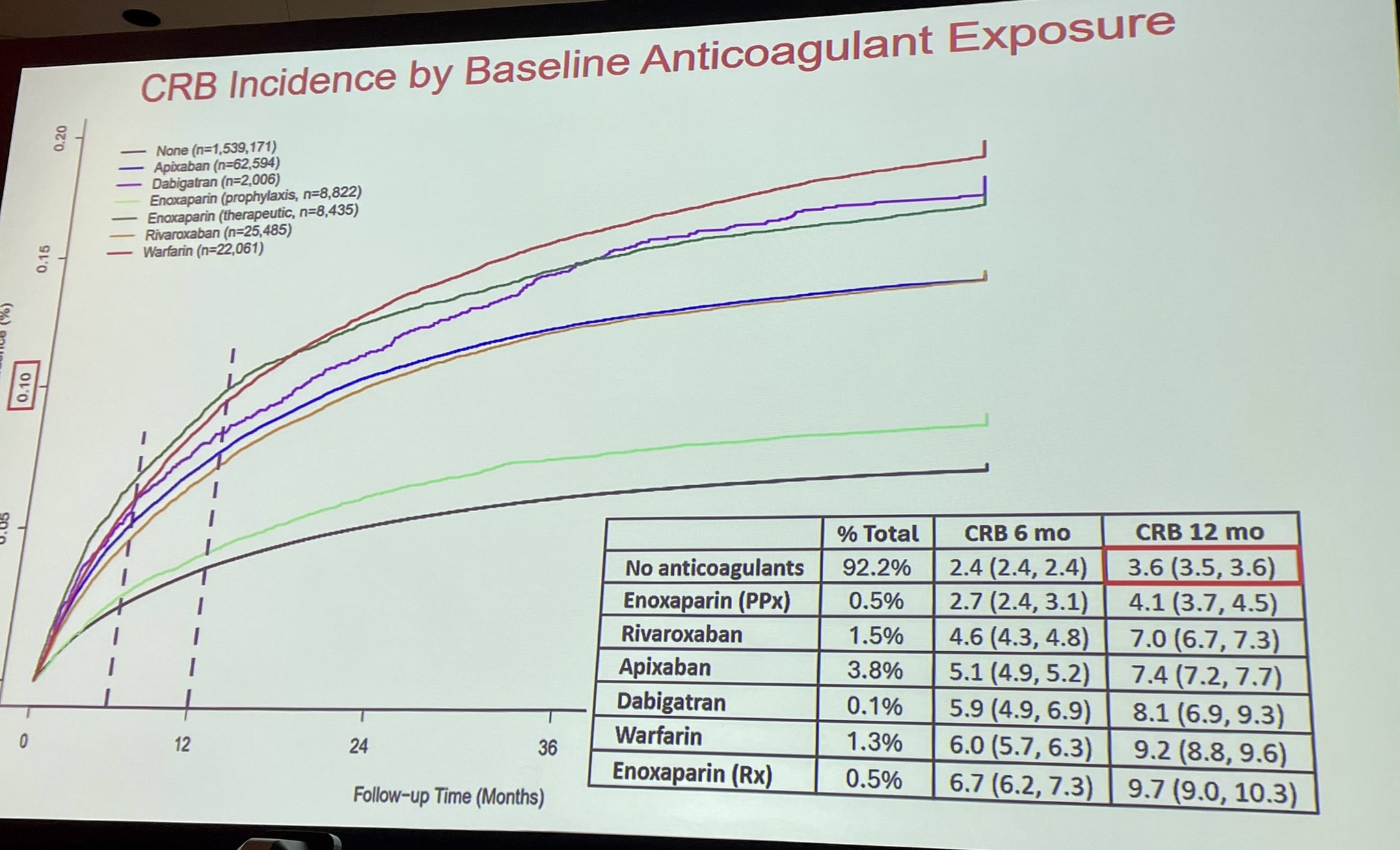
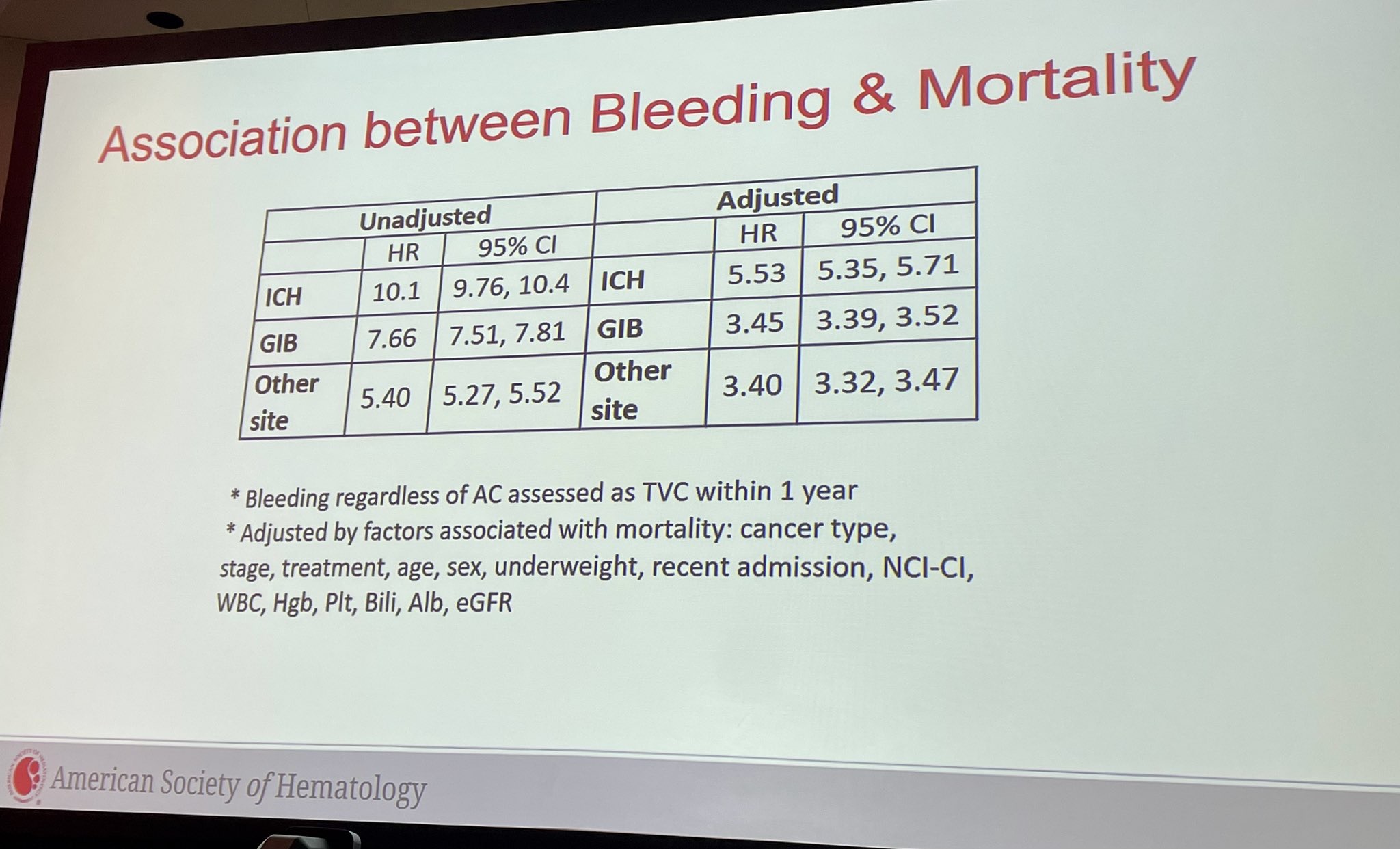
7.”Cancer-associated bleeding in the US: new data from >1.6M patients ASH25
• 12-mo bleeding: 3.9% overall; 4.5% with systemic therapy
• GI bleeds 2.1% most common; ICH 0.5% but deadly
• High-risk: leukemia, HCC, upper GI, brain mets
• ICH (HR 5.5) and GI bleed (HR 3.5) ↑ mortality
Read the full article by Ang Li and Colleagues here.
 ”
”
8.”Pregnancy-associated VTE and racial disparities at ASH25
In a population study of 442,816 pregnancies, 1,793 VTEs occurred (4.0/1,000).
Asian and Black individuals had lower VTE incidence (aRR 0.48 and 0.73) but more diagnostic delays plus higher acute-care use after VTE.
17-fold increase in ED visits in week pre-diagnosis
Read the full article by Yan Xu and Colleagues here.
 ”
”
All from ASH25 featured in Hemostasis Today.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-
Aug 11, 2026, 05:53Isaac Okello: Strengthening Sickle Cell Advocacy in Uganda
-
Aug 11, 2026, 05:38Rami Unterman: A Simple New Biomarker for Fibrotic ILDs
-
Aug 11, 2026, 04:10Haroun Gajraj: CLaCS vs Sclerotherapy – What Does the Evidence Show
-
Aug 11, 2026, 02:54Tareq Abadl: The Ultimate Guide to Clinically Significant Antibodies
-
Aug 10, 2026, 17:35Chokri Ben Lamine: Balancing Holistic Care and Precision in Hematology
-
Aug 10, 2026, 17:14Anna Stanizzi: Patient Blood Management as a New Model of Personalized Care
-
Aug 10, 2026, 17:12Odong Christopher: New Research on Ischemic Stroke Prediction in Uganda
-
Aug 10, 2026, 16:58Jeff Szer AM: Advancing the Management of Paroxysmal Nocturnal Hemoglobinuria
-
Aug 10, 2026, 16:51Suebsarn Ruksakulpiwat։ A New Milestone in the Development of the Stroke Risk Screening Scales