
Chokri Ben Lamine: Thread Platelet Subpopulations Leads to Therapeutic Implications
Chokri Ben Lamine, Adult Hematology and SCT Assistant Consultant at Oncology Center of Excellence at King Faisal Specialist Hospital and Research Center, shared a post on X:
“Thread Platelet Subpopulations Leads to Therapeutic Implications
(Focus: actionable strategies for hematologists ans cardiologists)
Credits: Dr. Alyamany
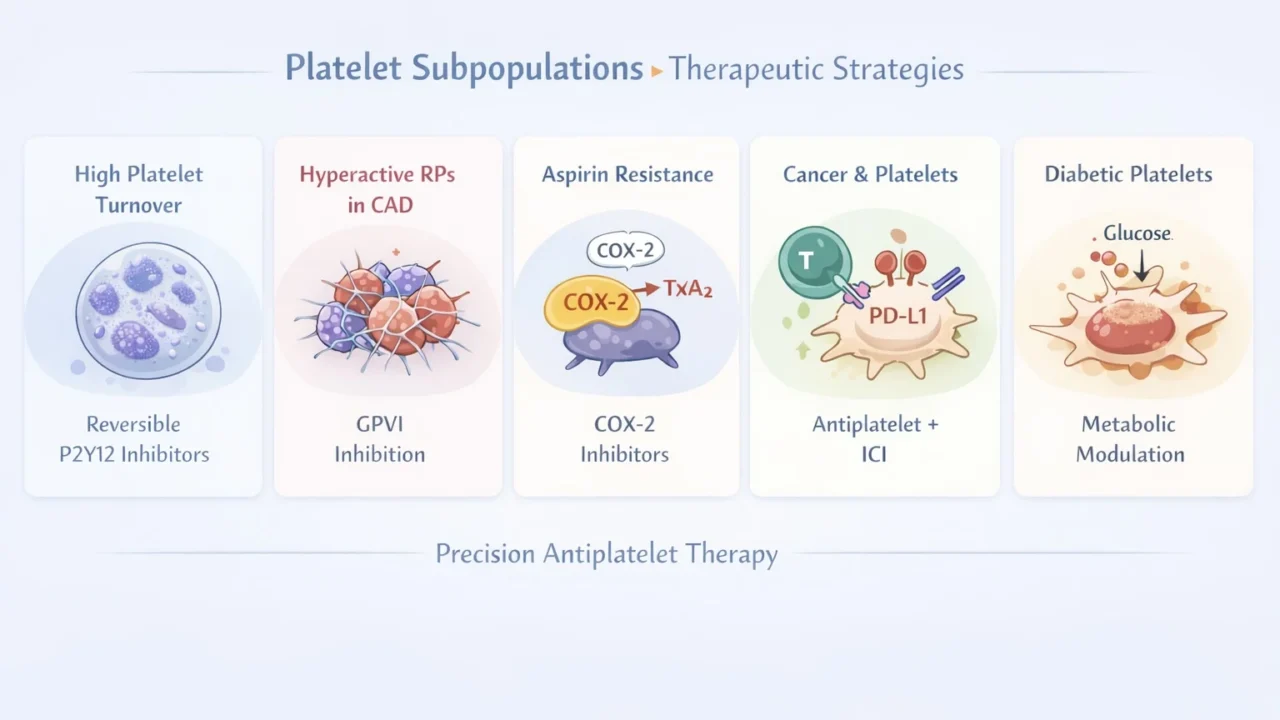
- High platelet turnover leads to increased reticulated platelets (RPs)
- Use reversible P2Y12 inhibitors (ticagrelor, cangrelor) instead of clopidogrel/prasugrel
- Continuous inhibition overcomes newly formed platelets escape
- PLATO: decreased death/MI/stroke but increased non-procedural bleeding
- Key concept: ‘platelet turnover: resistance to irreversible drugs’
Hyperreactive RPs in CAD
- Target pathways: GPVI inhibition (glenzocimab, revacept)
- with or without PI3K inhibition (LY294002 experimental)
- Mechanism: decreased collagen-driven activation and RP hyperreactivity
- Phase II PCI: safe with decreased bleeding but no clear MI reduction yet
- Future: selective anti-thrombotic without bleeding penalty
COX-2–mediated thromboxane (aspirin resistance biology)
- RPs express increased COX-2 so aspirin less effective
Strategy:
- Adjust aspirin dosing or COX-2 inhibition (e.g., celecoxib)
- Target: decreased TxA2 production in young platelets
- Evidence mixed, not standard yet
- Explains ‘high on-treatment platelet reactivity”\’
Cancer and immune evasion (PD-L1 positive platelets)
- Target axis:
- VEGF / PDGF inhibition
- alphaIIb beta3 blockade (eptifibatide)
- Mechanism: reverse platelet-mediated immunosuppression
- APOLLO (NSCLC): signal for increased PFS with antiplatelet plus ICI
- Platelets act as immune checkpoint modulators
Diabetes-associated platelet dysfunction
- Hyperglycemia leads to increased S100A8/A9 leads to increased TPO leads to increased RPs leads to thrombosis
- Therapeutic strategies:
- SGLT2 inhibitors (decrease RP production indirectly)
- S100A8/A9 inhibitors (ABR-215757)
- IL-6 / TPO modulation
- Result: decreased platelet hyperreactivity and restored antiplatelet response
- Precision approach: treat metabolism to fix platelets
Core clinical takeaways
- Not all platelets are equal: ‘subpopulation-driven thrombosis’
- Young platelets: drug resistance and higher risk
- Future: target biology (GPVI / S100A8/A9 / PD-L1) not just aggregation
- Move from ‘one-size antiplatelet’ to precision platelet therapy
MCQ
Which strategy best overcomes high platelet turnover–related resistance?
- Increase aspirin dose
- Switch to clopidogrel
- Use ticagrelor
- Add warfarin
Answer: C
Reversible P2Y12 inhibition maintains effect despite new platelet generation
OSCE scenario
Post-PCI patient with recurrent events despite DAPT and high IPF%
- Best step: switch to ticagrelor-based strategy
- Consider future: GPVI-targeted therapy (trial setting).”

Find more posts featuring Chokri Ben Lamine on Hemostasis Today.
-
Jul 14, 2026, 12:08Elvira Grandone: Finding the Right LMWH Dose for Pregnant Patients Suffering From DVT
-
Jul 14, 2026, 12:05Eloïse Laouenan: From Washington to Paris – Join GETBO at ISTH 2026
-
Jul 14, 2026, 12:02Louise St. Germain Bannon: Our first ISTH regulatory session at ISTH 2026
-
Jul 14, 2026, 11:21Malwina Maliszewska: Advancing Coagulation Diagnostics at ISTH 2026
-
Jul 14, 2026, 11:07Mary Cushman: Honoring Outstanding Mentorship at ISTH 2026
-
Jul 14, 2026, 10:53Maha Othman: Advancing the Management of Inherited Thrombocytopenias at ISTH 2026
-
Jul 14, 2026, 10:24Sara Zalghout: The Little Things That Make ISTH 2026 Special
-
Jul 14, 2026, 10:11Joseph R. Shaw: GAUGE Advances FXa Inhibitor Reversal at ISTH 2026
-
Jul 13, 2026, 23:39Yaariv Khaykin: Whole-Person Care Can Strengthen Stroke Prevention in Patients With Atrial Fibrillation