
Alisha Tuck: Ultrasound and Anticoagulation Management in Pregnancy – Why Anticoagulation Matters?
Alisha Tuck, Obstetrics and Gynecology Sonographer at Sonopartners, LLC, shared a post on LinkedIn:
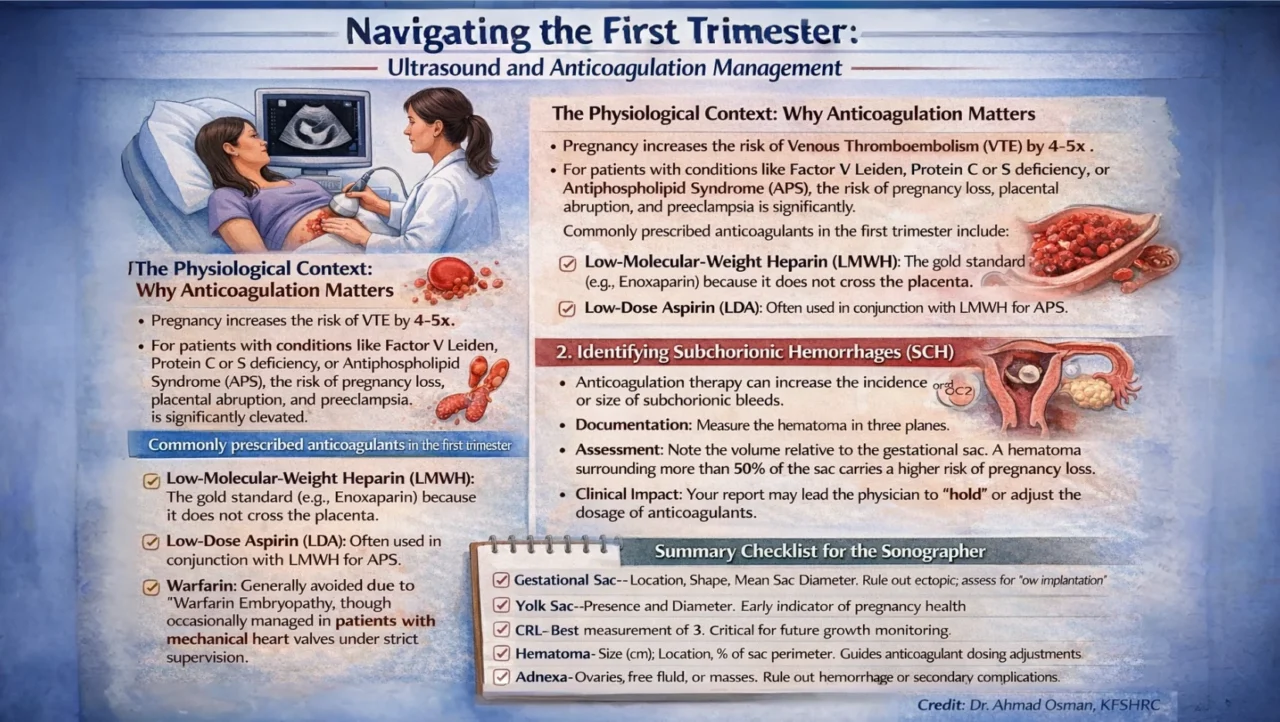
“Navigating the First Trimester: Ultrasound and Anticoagulation Management
The Physiological Context: Why Anticoagulation Matters
Pregnancy increases the risk of Venous Thromboembolism (VTE) by 4-5x .
For patients with conditions like Factor V Leiden, Protein C or S deficiency, or Antiphospholipid Syndrome (APS), the risk of pregnancy loss, placental abruption, and preeclampsia is significantly elevated.
Commonly prescribed anticoagulants in the first trimester include:
- Low-Molecular-Weight Heparin (LMWH): The gold standard (e.g., Enoxaparin) because it does not cross the placenta.
- Low-Dose Aspirin (LDA):Often used in conjunction with LMWH for APS.
- Warfarin: Generally avoided due to ‘Warfarin Embryopathy,’ though occasionally managed in patients with mechanical heart valves under strict supervision.
Key Sonographic Objectives in the First Trimester
When scanning a patient on anticoagulation, our focus shifts toward identifying early signs of pregnancy failure or maternal complications.
1. Confirming Viability and Dating
Accurate dating is paramount.
In patients with clotting disorders, placental insufficiency can manifest later; having a rock – solid CRL from the first trimester ensures that later growth restrictions are identified promptly.
2. Identifying Subchorionic Hemorrhages (SCH)
Anticoagulation therapy can increase the incidence or size of subchorionic bleeds.
- Documentation: Measure the hematoma in three planes.
- Assessment: Note the volume relative to the gestational sac. A hematoma surrounding more than 50% of the sac carries a higher risk of pregnancy loss.
- Clinical Impact: Your report may lead the physician to ‘hold’ or adjust the dosage of anticoagulants.
3. Corpus Luteum and Adnexal Evaluation
Check for large corpus luteum cysts or evidence of internal hemorrhage.
While common, anticoagulated patients are at a slightly higher risk for hemorrhagic cysts, which can mimic ectopic pregnancy symptoms (pelvic pain).
Summary Checklist for the Sonographer
- Gestational Sac – Location, Shape, Mean Sac Diameter. Rule out ectopic; assess for ‘low implantation’
- Yolk Sac – Presence and Diameter. Early indicator of pregnancy health
- CRL – Best measurement of 3 | Critical for future growth monitoring
- Hematoma – Size (cm), Location, % of sac perimeter. Guides anticoagulant dosing adjustments
- Adnexa – Ovaries, free fluid, or masses. Rule out hemorrhage or secondary complications
Conclusion
Sonographers play a pivotal role in the multidisciplinary care of the high – risk obstetric patient.
By providing meticulous documentation of the early pregnancy and any associated perigestational bleeding, we allow the clinical team to tailor anticoagulation therapy – optimizing the safety of both the mother and the developing embryo.”

Stay updated with Hemostasis Today.
-
Jul 17, 2026, 10:12Julien Perrin: Presenting Thalassemia Coagulation Research at ISTH 2026
-
Jul 17, 2026, 10:08Cihan Ay: Thank you for making ISTH 2026 such a remarkable congress
-
Jul 17, 2026, 10:06Laura Cunliffe: That Is a Wrap for Meg and Me at ISTH 2026 in Paris
-
Jul 17, 2026, 10:03Roberta Gualtierotti: Updating on the Standardization of ultrasound definitions in hemophilic arthropathy at the ISTH 2026
-
Jul 17, 2026, 09:57Hrushikesh Vyas – A Wonderful Week Presenting Inherited Thrombocytopenia Research at ISTH 2026
-
Jul 17, 2026, 09:42Samin Mohsenian: Proud to Receive a Top Poster Award at ISTH 2026
-
Jul 17, 2026, 09:36Wolfgang Miesbach: A Landmark Case of Supratherapeutic FIX Following Gene Therapy Presented at ISTH 2026
-
Jul 17, 2026, 09:28Lisa Astorga: Leaving ISTH 2026 Inspired by the Global Thrombosis and Hemostasis Community
-
Jul 17, 2026, 09:23Maxime Dely: Honored to Reach My 6th Plasma Donation of 2026