

Amelia Carro Hevia: Effect of Alirocumab on Coronary Plaque After MI
Amelia Carro Hevia, Consultant Cardiologist and Researcher at Corvilud Institut, shared a post on LinkedIn:
“Alirocumab and coronary plaque after myocardial infarction (MI): who really benefits?
Context
After an acute MI, patients remain at increased residual risk despite high intensity statin therapy.
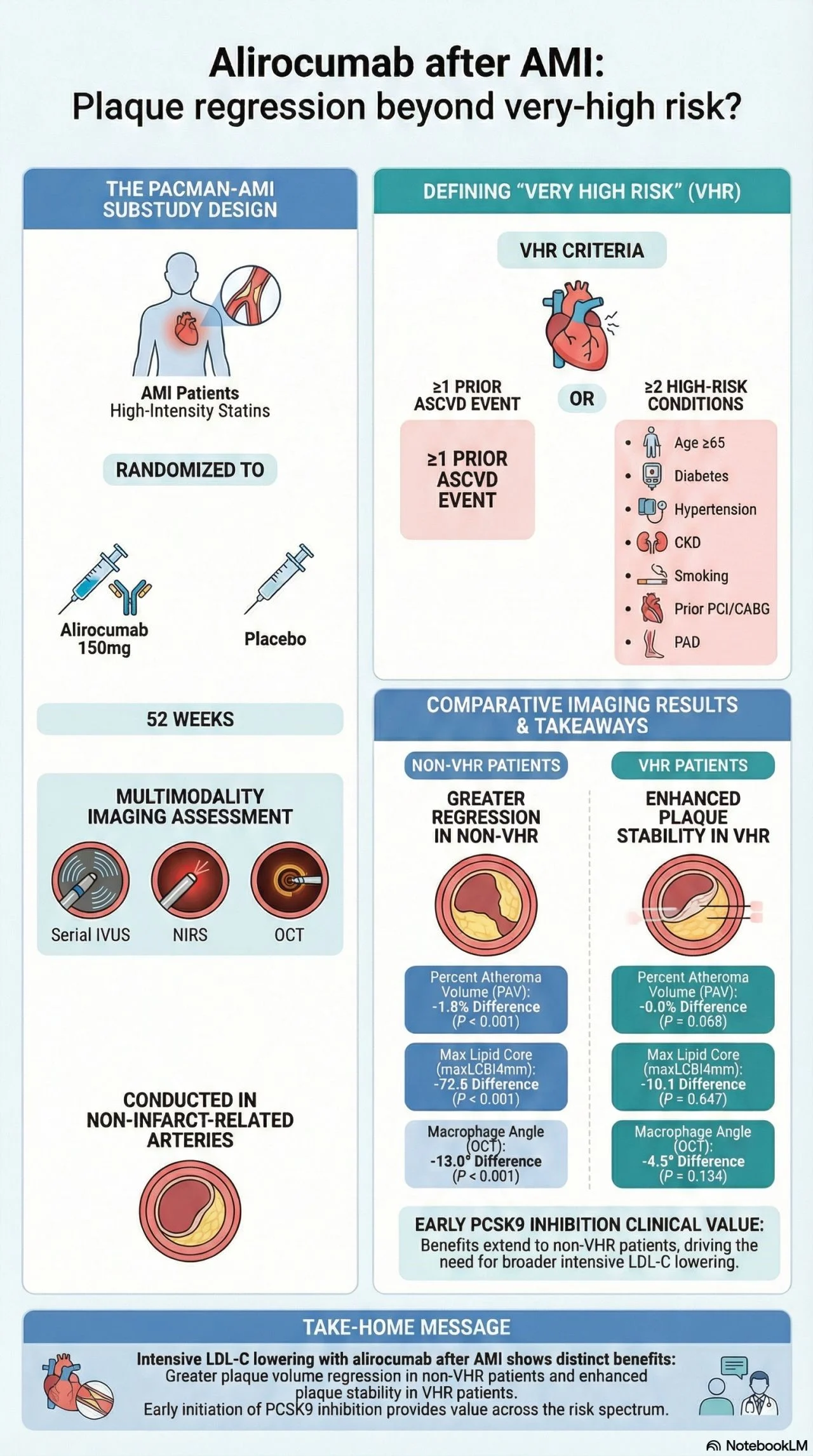
Adding the PCSK9 inhibitor alirocumab on top of statins promotes coronary plaque regression and stabilization in PACMAN‑AMI.
This new substudy asks a clinically relevant question:
Does the effect on plaque regression differ according to the number of atherothrombotic risk enhancers?
Study at a glance
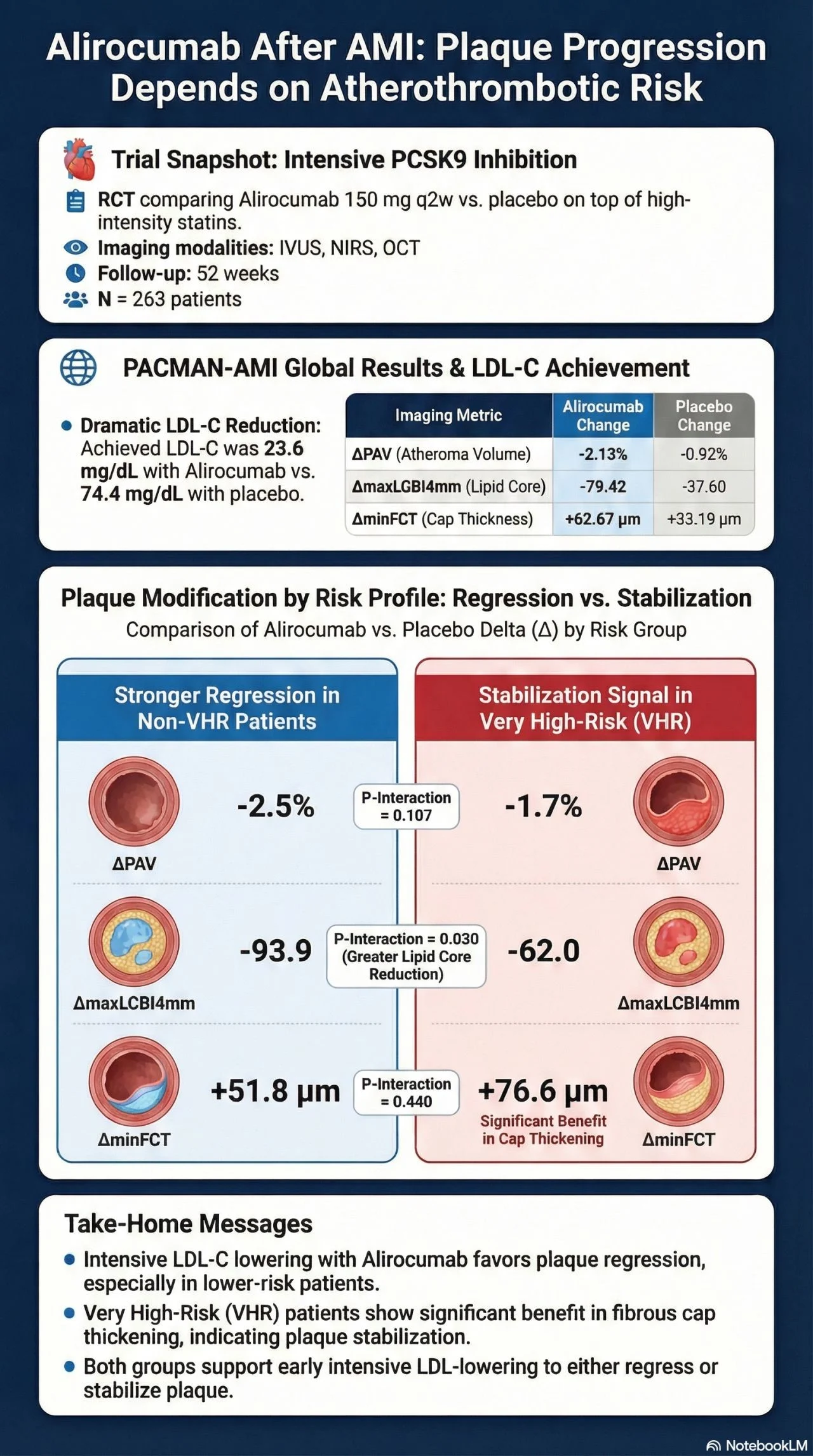
Design: substudy of PACMAN‑AMI, randomized, double‑blind, alirocumab 150 mg q2w vs placebo plus high intensity statin for 52 weeks.
Population: 263 MI patients with serial IVUS in non‑culprit arteries.
Risk stratification: number of ACC/AHA atherothrombotic risk enhancers (prior MI/stroke/PAD, age greater than or equal to 65, FH, revascularization, diabetes, HTN, CKD, smoking, LDL‑C greater than or equal to 100 mg/dL on max statin, HF).
- 0 risk factors (n equals 52)
- 1 risk factor (n equals 101)
- greater than or equal to 2 risk factors (n equals 100)
1ARY endpoint: change in % atheroma volume (PAV) by IVUS from baseline to 52 weeks
Main findings
1.More risk factors more plaque at baseline
Baseline PAV: 39.0% (0 RF) vs 42.6% (1 RF) vs 42.8% (greater than or equal to 2 RF), p equals 0.008
Patients with multiple risk enhancers already have more advanced atheroma
2. Alirocumab plus statin leads to greater plaque regression in low‑to‑intermediate risk
0 risk factors: PAV change
- Alirocumab: −2.66% vs placebo: −1.02%, p equals 0.009.
1 risk factor: - Alirocumab: −2.36% vs placebo: −0.76%, p less than 0.001
Stronger plaque regression with alirocumab when patients have 0-1 atherothrombotic enhancer.
3. Greater than or equal to 2 risk factors: no significant incremental regression
Greater than or equal to 2 risk factors:
Alirocumab: −1.72% vs placebo: −1.12%, p equals 0.076; p for interaction equals 0.009
In patients with multiple risk enhancers, adding alirocumab did not significantly increase plaque regression vs statin alone
4. Plaque biology/timing matter
Results complement prior PACMAN‑AMI analyses showing that:
- Very low on‑treatment LDL‑C is associated with more regression and fibrous cap thickening.
- Lesions with increased baseline plaque burden & more lipid show more regression and stabilization with alirocumab
- Global atherothrombotic burden seems to attenuate the imaging benefit.
Clinical ‘messages to go’
Alirocumab after MI
Promotes coronary plaque regression, but the biggest IVUS benefit is seen in patients with 0–1 atherothrombotic risk enhancer
Multiple risk enhancers (greater than or equal to2) euals higher plaque burden, but less additional regression with alirocumab vs statins in this 1‑year window
Risk scores vs biology: traditional risk enrichment (more RF equals increased clinical risk) may not mirror plaque‑level responsiveness to PCSK9 inhibition.
Mechanistic data (PACMAN‑AMI, ARCHITECT, ALTAIR) consistently show regression and stabilization with PCSK9 inhibitors, but patient selection and timing could be key
These findings support early, intensive LDL‑C lowering post‑MI, but invite reflection on which patients gain the most plaque‑level benefit and for how long.”

Stay updated with Hemostasis Today.
{kind=link}
{kind=link}
-
Jul 19, 2026, 06:28Estrogen-Associated VTE: From Real-World Evidence to the Biology of Persistent Thrombosis
-
Jul 19, 2026, 05:01Maissa El-Qendouci: Optimizing Iron Deficiency Diagnosis in TAVR
-
Jul 19, 2026, 04:39Saoud Hassan: Identifying Monocytic Precursors Under the Microscope
-
Jul 19, 2026, 04:23Iris van Moort: Expert Insights on Pediatric Hemostasis Diagnostics at ISTH 2026
-
Jul 19, 2026, 04:09Er. Subodh Grewal: How Platelet Histograms Support Hematology Diagnosis
-
Jul 19, 2026, 03:53Serhii Pelishenko: Current Evidence on Kaolin and Chitosan Dressings
-
Jul 18, 2026, 23:52Chinua Onyebuchi: Applications Now Open for the European Stroke Master Programme
-
Jul 18, 2026, 22:43Exploring the Ultra-Late Window for Stroke Treatment – International Journal of Stroke
-
Jul 18, 2026, 21:38Swastik Sharma Deviprasad Bhat: A One-Minute Guide to Recognizing Stroke