
Apr 1, 2026, 17:15
Chokri Ben Lamine: Differentiating Reactive from Clonal Causes in Adult Neutrophilia
Chokri Ben Lamine, Adult Hematology and SCT Assistant Consultant at Oncology Center of Excellence at King Faisal Specialist Hospital and Research Center, shared a post on X:
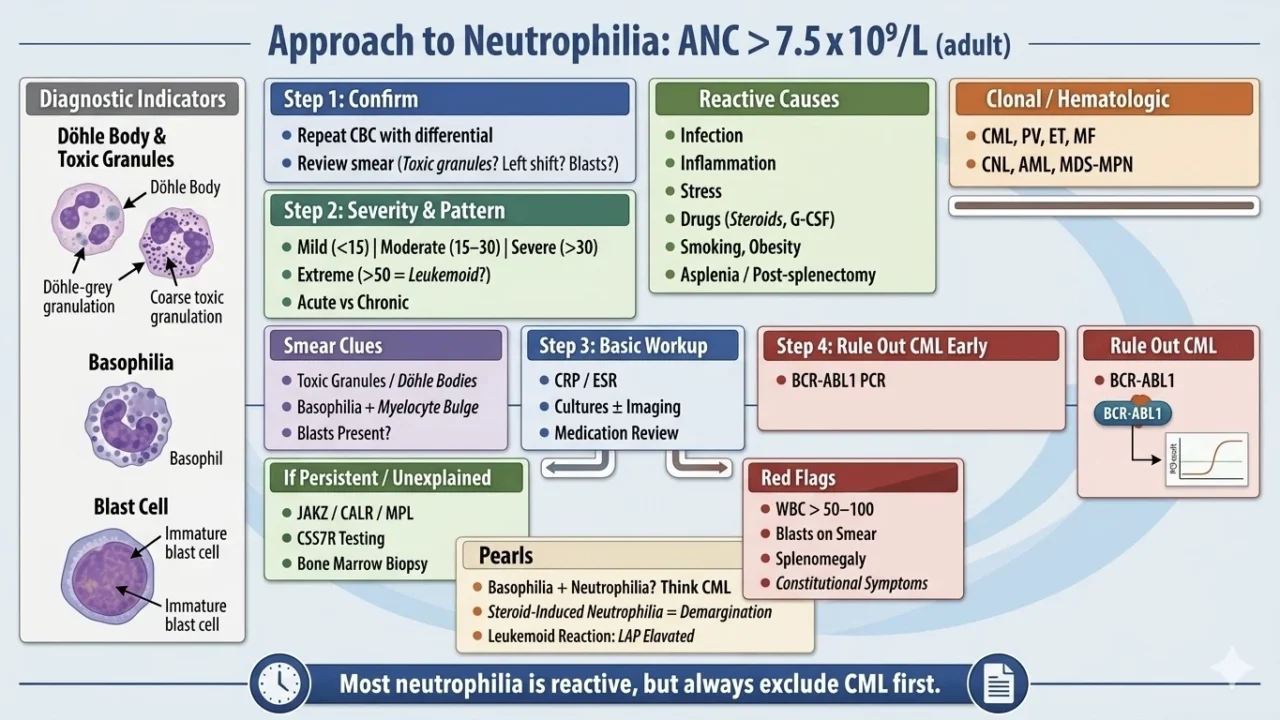
“Neutrophilia approach: ANC greater than 7.5 ×10⁹/L (adult) should be classified reactive vs clonal
Step 1: confirm
- repeat CBC with differential
- review smear (toxic granulation? left shift? blasts?)
Step 2: severity and pattern
- mild (<15) | moderate (15–30) | severe (>30) | extreme (>50 = leukemoid?)
- acute vs chronic
Reactive causes (most common)
- infection (bacterial, severe viral early)
- inflammation (RA, IBD, vasculitis)
- stress (trauma, surgery, MI)
- drugs (steroids, G-CSF, lithium)
- smoking, obesity
- asplenia/post-splenectomy
Clonal / hematologic
- MPN: CML, PV, ET, MF
- CNL (rare, CSF3R+)
- AML with leukocytosis
- MDS/MPN overlap
Smear clues
- toxic granulation/Döhle bodies indicates a reactive
- basophilia with myelocyte bulge then think CML
- blasts raise concern for acute leukemia
Step 3: basic workup
- CRP/ESR
- cultures ± imaging if infection suspected
- medication review
Step 4: rule out CML early
BCR-ABL1 PCR (must not miss)
If persistent/unexplained
- JAK2 / CALR / MPL
- CSF3R if CNL suspected
- bone marrow biopsy
Red flags (urgent)
- WBC greater than 50–100
- blasts on smear
- organomegaly
- constitutional symptoms
Pearls
- neutrophilia with basophilia should be considered CML until proven otherwise
- steroid-induced neutrophilia results from demargination (no left shift)
- leukemoid reaction can mimic leukemia but LAP high
One-liner
most neutrophilia is reactive, but always exclude CML first”
Stay updated with Hemostasis Today.
-
Jul 7, 2026, 17:14Shabneez Hussain: Blood Transfusion Professionals Connecting at ISBT 2026
-
Jul 7, 2026, 17:04Mariam Swidan: Vitamin B12 Deficiency and the Hidden Risk of Neurological Damage
-
Jul 7, 2026, 16:53Heghine Khachatryan: Breaking Barriers in Bleeding Disorder Care for Women and Girls
-
Jul 7, 2026, 16:39Why Medical Alert Identification Matters in Bleeding Disorders – South African Haemophilia
-
Jul 7, 2026, 16:21Hannah Omunakwe: When Blood Becomes the Limiting Treatment in Sickle Cell Disease
-
Jul 7, 2026, 15:54Barbara Lovrencic: Giving the ITP Patient Voice a Stronger Evidence Base
-
Jul 7, 2026, 15:45Maria Cherska: Can Cardiovascular Prevention Become Truly Personalized If We Ignore Ethnicity?
-
Jul 7, 2026, 15:42Julie Makani: The London Patient – A Milestone in HIV Cure
-
Jul 7, 2026, 15:39July Issue is Now Live – The Lancet Haematology