

Heghine Khachatryan: ISTH 2026 – Final Day Highlights
Heghine Khachatryan, Editor-in-Chief of Hemostasis Today, Head of Hemophilia and Thrombosis Center at Yeolyan Hematology and Oncology Center, shared a post on LinkedIn:
“ISTH 2026 | Final Day Highlights
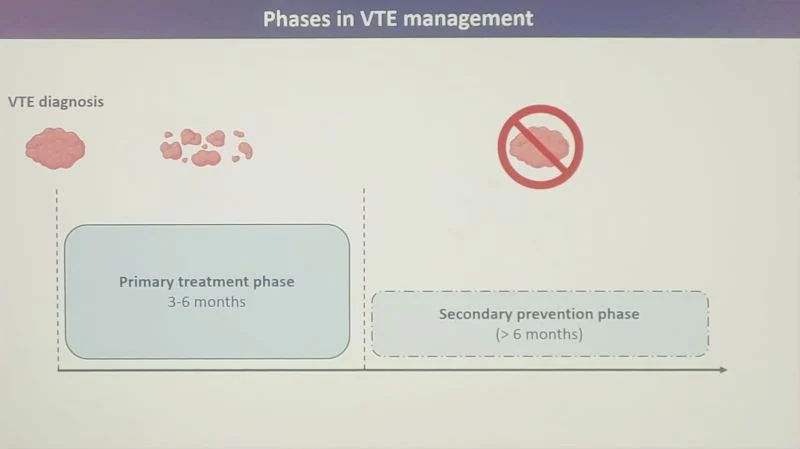
Estrogen-associated venous thromboembolism: Is less anticoagulation enough?
One of the most thought-provoking presentations on the final day of ISTH 2026 addressed a clinically important but often under-discussed question:
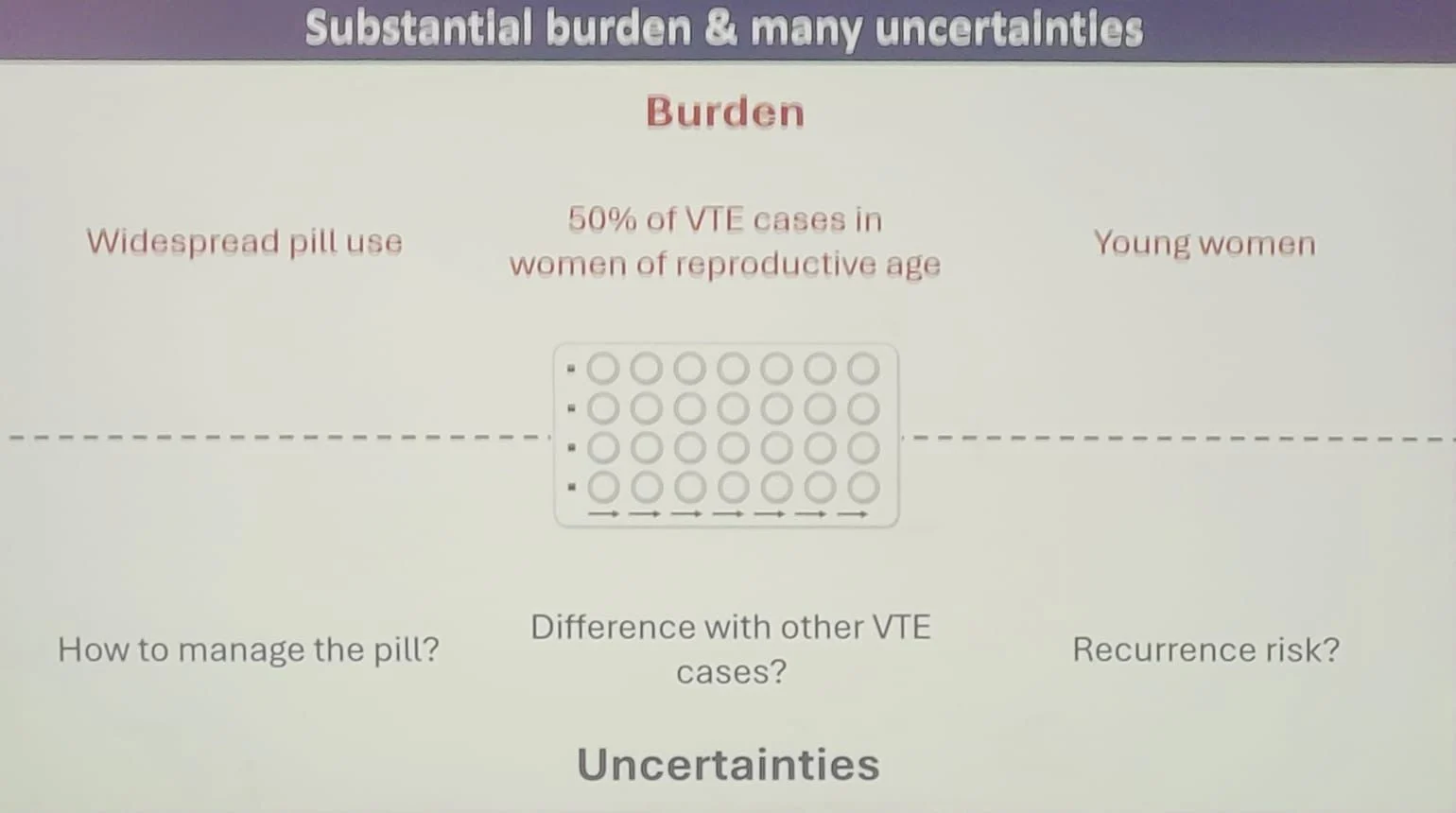
Should estrogen-associated venous thromboembolism (VTE) be managed differently from other provoked VTE events?
Dr. Andreas Verstraete presented data from the RIETE Registry, one of the world’s largest prospective VTE registries, evaluating the presentation, treatment, bleeding risk, and recurrence patterns in women with estrogen-associated thrombosis.
Study population
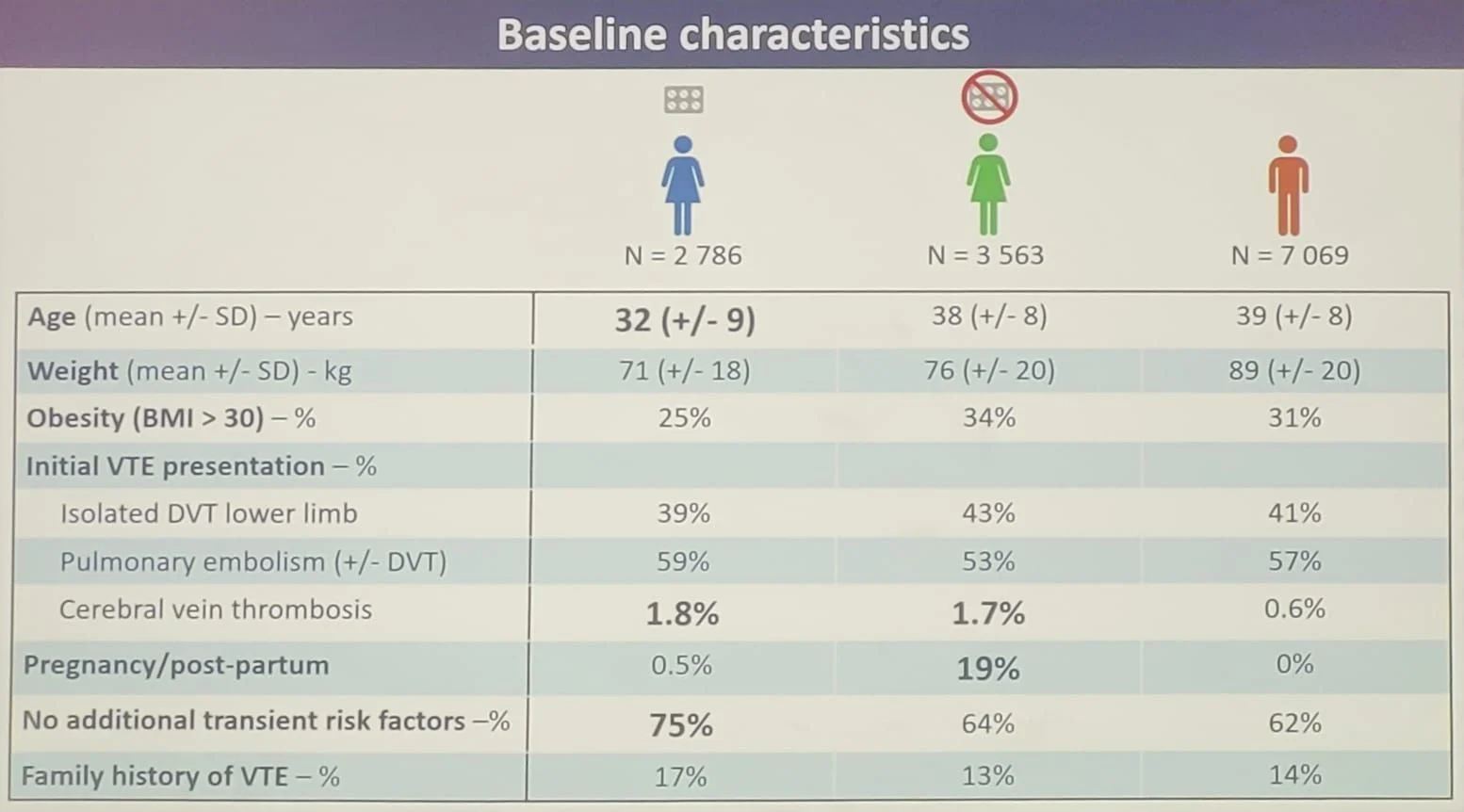
The analysis included 13,418 patients aged 10–49 years diagnosed with lower-extremity DVT, pulmonary embolism (PE), cerebral venous thrombosis (CVT), or superficial vein thrombosis (SVT):
- 2,786 women with estrogen-associated VTE
- 3,563 women with non-estrogen-associated VTE
- 7,069 men with VTE
Patients with active cancer, older age, and other uncommon thrombosis sites were excluded, allowing a focused comparison of hormonally provoked thrombosis.
Key baseline observations
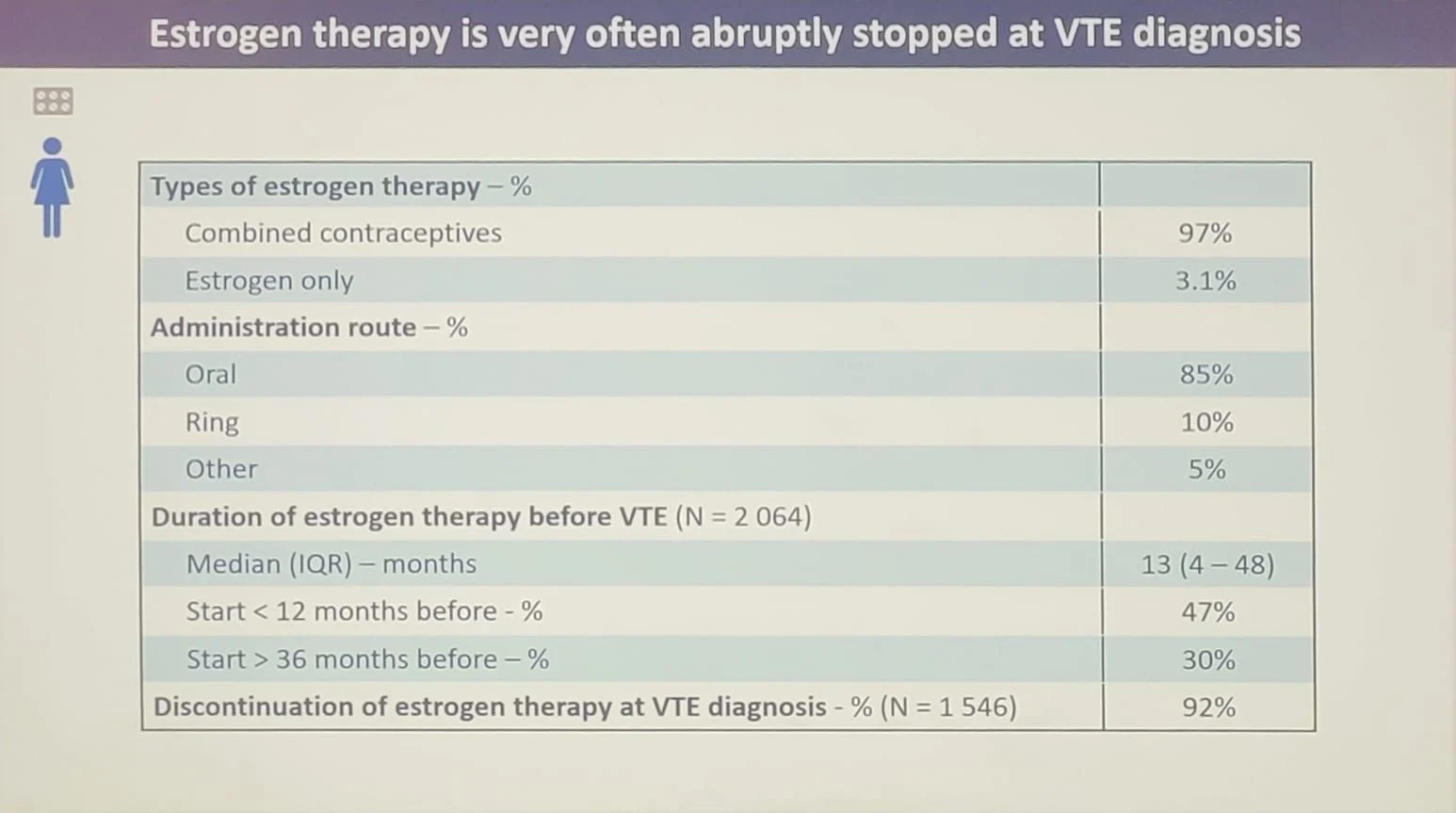
Women with estrogen-associated VTE represented a distinct clinical phenotype:
- They were substantially younger (mean age 32 years) than women without estrogen exposure (38 years) and men (39 years).
- Nearly three-quarters (75%) had no additional transient provoking factor, suggesting that estrogen exposure itself was frequently the only identifiable trigger.
- Pulmonary embolism
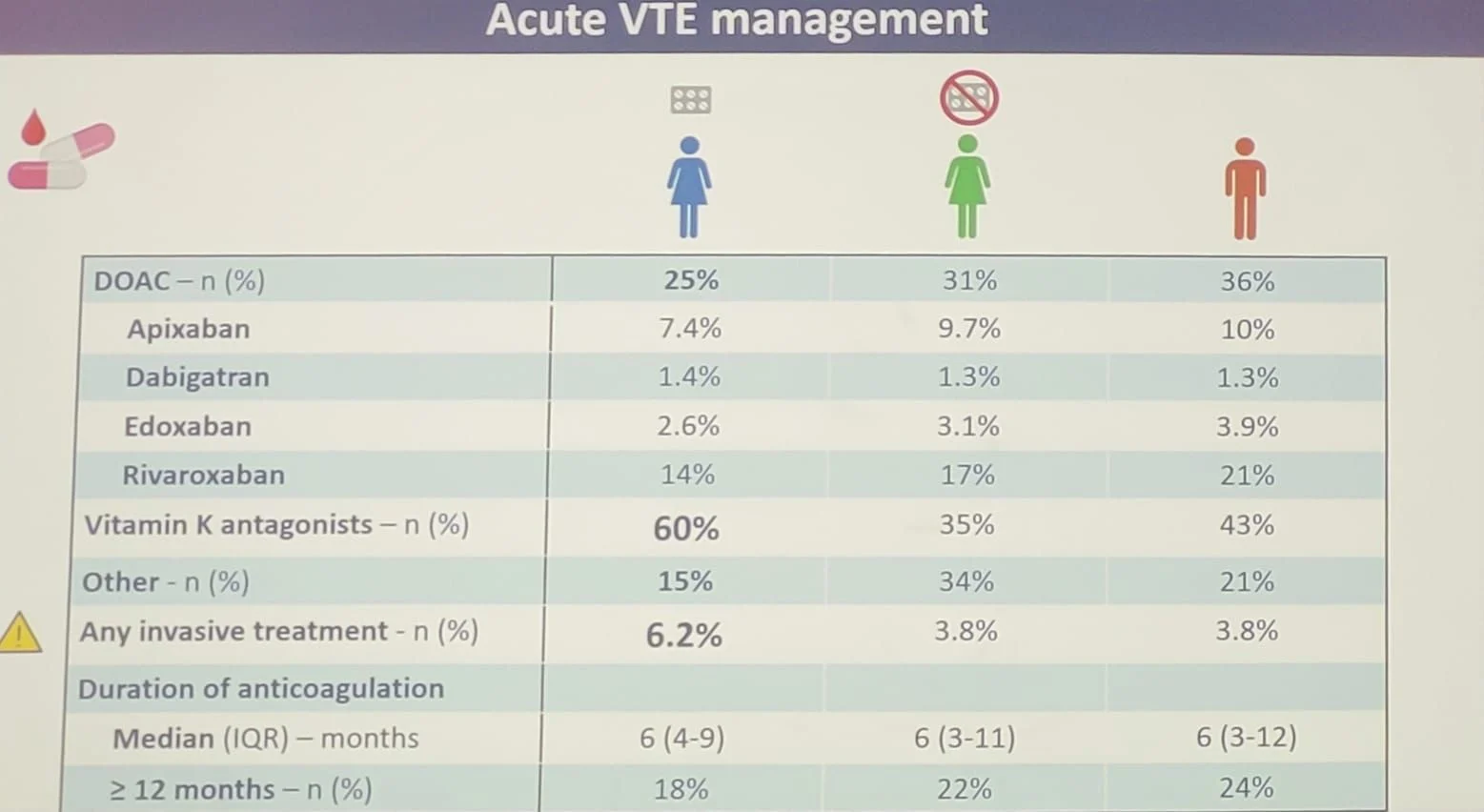
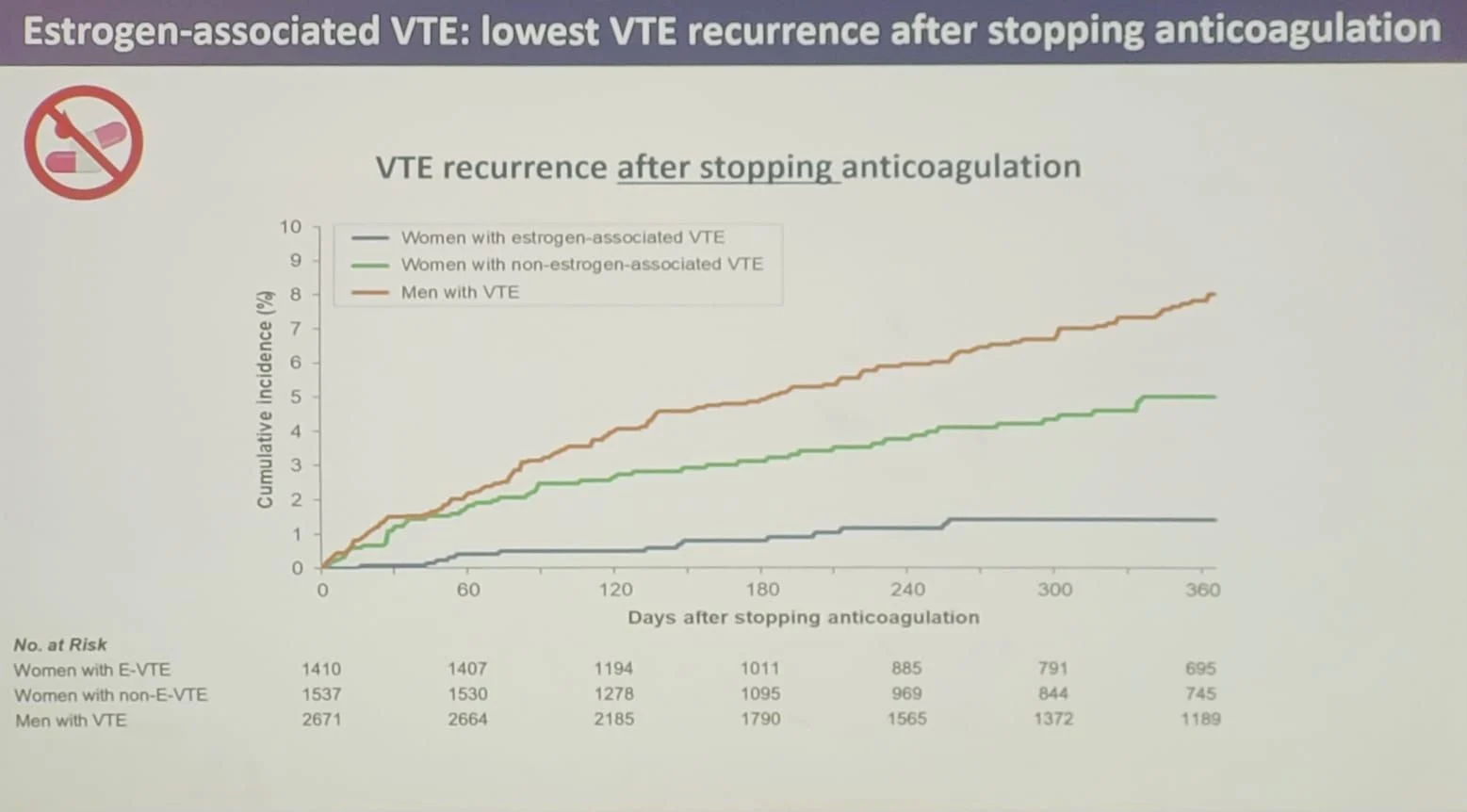
The RIETE data reinforce an increasingly accepted concept:
For women whose VTE is clearly provoked by estrogen exposure, and in whom the provoking factor has been discontinued, extended anticoagulation beyond the initial treatment phase is unlikely to provide substantial additional benefit for most patients.
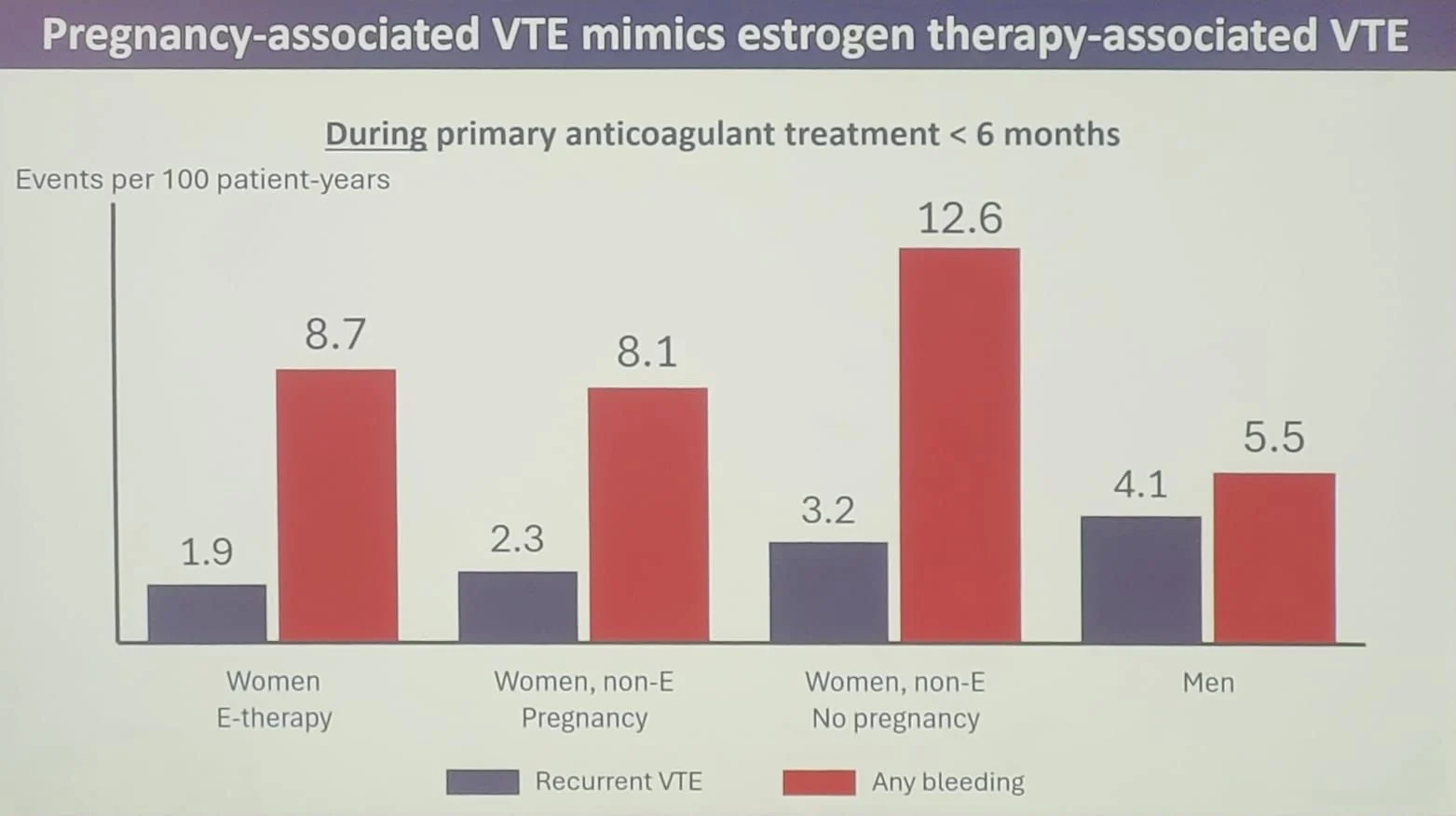
Instead, the decision should balance:
- the very low recurrence risk after stopping therapy,
- the measurable bleeding risk while continuing anticoagulation,
- patient preferences,
- future pregnancy plans,
- inherited thrombophilia,
- and persistent risk factors.
Importantly, the authors emphasized that long-term recurrence remains insufficiently characterized, highlighting the need for extended follow-up studies before definitive recommendations can be made.
Take-home message
This presentation provides robust real-world evidence that estrogen-associated VTE represents a unique clinical entity rather than simply another provoked thrombotic event.
Women with estrogen-associated thrombosis are younger, usually have estrogen exposure as the only identifiable provoking factor, experience the lowest recurrence rates after treatment discontinuation, and may derive limited benefit from prolonged anticoagulation.”

Stay Updated with the Latest ISTH 2026 Updates on Hemostasis Today.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-
Jul 18, 2026, 18:00Karen Schreiber: Advancing Thrombosis Epidemiology Through Global Collaboration at ISTH 2026
-
Jul 18, 2026, 17:34Living With ITP – A New Resource for Navigating Your Diagnosis – ITP Support Association
-
Jul 18, 2026, 17:34Mona Alfaraj: It Was a Hot Week Attending ISTH 2026 Congress in Paris
-
Jul 18, 2026, 17:26Shernan Holtan: Latest Publication on PTCy
-
Jul 18, 2026, 17:20Doaa EL Demerdash: Connecting the Global ITP Community at ISTH 2026
-
Jul 18, 2026, 16:58Isabella Presch: Innovative Trial Designs for Rare Pediatric Studies
-
Jul 18, 2026, 16:36Caitlin Schneider: Research, Collaboration, and New Beginnings at ISTH 2026
-
Jul 18, 2026, 16:23Panagiota Tsiatsiou: Honored to Present Our Research at the ISTH 2026 Congress in Paris
-
Jul 18, 2026, 16:03Robert Tadevosyan: A Week of Science, Collaboration, and Growth at ISTH 2026