
Yves Bikorimana: When More Is Not Better – Polycythemia
Yves Bikorimana, CEO at MedData – Rwanda and Lab Scientist at The University Teaching Hospital of Kigali – Chuk, shared a post on Linkedin:
“Polycytemia: When more is not better
Polycythemia is a hematological condition characterized by an abnormal increase in red blood cell (RBC) mass, resulting in increased blood viscosity and a heightened risk of vascular complications.
From a biological perspective, this elevated RBC count thickens the blood, impairing normal flow dynamics and predisposing individuals to thrombosis (clot formation).
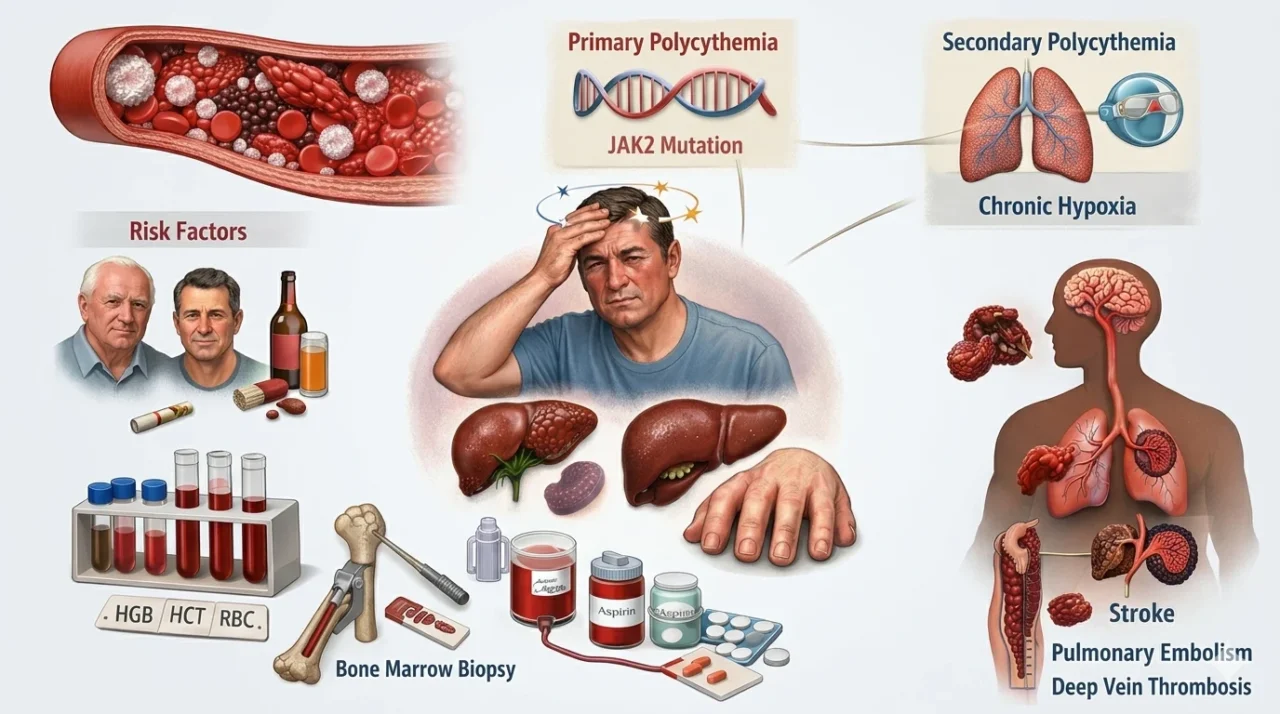
In many cases, white blood cells (WBCs) and platelets are also elevated, further amplifying the risk of complications.
Polycythemia can be broadly classified into two types.
Primary polycythemia, also known as polycythemia vera, is driven by mutations in the JAK2 gene, leading to uncontrolled RBC production independent of normal physiological regulation.
In contrast, secondary polycythemia arises due to chronic hypoxia (low oxygen levels), commonly associated with conditions such as lung disease, obesity, and smoking.
Several risk factors are associated with polycythemia, including age above 50 years, male predominance, radiation or toxin exposure, and chronic hypoxic conditions such as chronic obstructive pulmonary disease (COPD) and cardiovascular disorders. Lifestyle factors like smoking and alcohol use also contribute significantly.
Clinically, patients may present with symptoms such as headache, dizziness, fatigue, a flushed or ruddy complexion, and pruritus, particularly after warm showers. In more advanced or chronic cases, splenomegaly, hepatomegaly, and finger clubbing may also be observed.
Diagnosis is typically established through laboratory findings showing elevated hemoglobin (HGB), hematocrit (HCT), and RBC count, often accompanied by increased WBCs and platelets. Confirmation may involve JAK2 mutation testing, bone marrow biopsy, and imaging studies to identify underlying secondary causes.
If left unmanaged, polycythemia can lead to serious complications, including thrombosis (such as stroke, deep vein thrombosis, and pulmonary embolism), myelodysplastic syndromes, and in some cases progression to acute leukemia.
Management strategies focus on reducing RBC mass and preventing thrombotic events. Therapeutic approaches include phlebotomy to decrease blood volume, hydroxyurea to suppress RBC production, and low-dose aspirin to reduce clotting risk. Adequate hydration is also essential to help lower blood viscosity.
Polycythemia highlights a fundamental principle in physiology: homeostasis depends on balance, not excess. Even essential components like red blood cells can become harmful when dysregulated.
Early recognition and timely intervention are therefore critical in preventing life-threatening outcomes, while advances in molecular understanding, particularly involving JAK2 mutations, continue to shape targeted therapies in modern hematology.”

Stay updated with Hemostasis Today.
-
Jul 4, 2026, 17:38Michael Stark: Greater Improvements in Cerebral Oxygenation With Restrictive Transfusion Thresholds
-
Jul 4, 2026, 17:27Reza Shojaei: How America Won the Plasma Race
-
Jul 4, 2026, 17:26Akshat Jain: The First CRISPR-Cas9 Gene Therapy Approved for Children as Young as 2 with SCD
-
Jul 4, 2026, 17:25Francesca Palandri: Dynamic, Treatment Response-Driven Risk Assessment in Polycythemia Vera
-
Jul 4, 2026, 17:24Thierry Burnouf: The Fragile Supply of Human Hyperimmune Immunoglobulins
-
Jul 4, 2026, 15:41Emmanuel J. Favaloro: New Research Highlights Benchmarks for Low Molecular Weight Heparin Monitoring
-
Jul 4, 2026, 15:38Roshni Kulkarni: Maternal Mortality In Bleeding Disorders
-
Jul 4, 2026, 15:34Alejandro González Veliz: Does Elevated Lp(a) Always Mean the Same Cardiovascular Risk?
-
Jul 4, 2026, 15:20Bruno Pougault: Heparin Monitoring Remains One of the Most Challenging Areas in Laboratory Hemostasis