
Abdulaziz (Omar) Badran: Our Case Contain Very Strange and Rare Combination of 2 Causes of Hemolytic Anemia
Abdulaziz (Omar) Badran, Hematology Supervisor at Almoosa Specialist Hospital, shared an interesting case on LinkedIn:
“Good evening to all , our case today contain very strange and rare combination of 2 causes of hemolytic anemia . First this 35 years male came to ER with very strong body pain , fatigue, pale color and dark urine that he noticed . The CBC showed Marked severe anemia with Macrocytic RBCs and normal WBCs with normal platelet count . Also very high Retics and bilirubin honestly at the begening I thought it’s sickle cell crisis , very low HGB , high MCV and high Retics . Then we after checking his history I found he is negative for sickle and his last CBC had much higher HGB with 11.3 and now 5.06 only
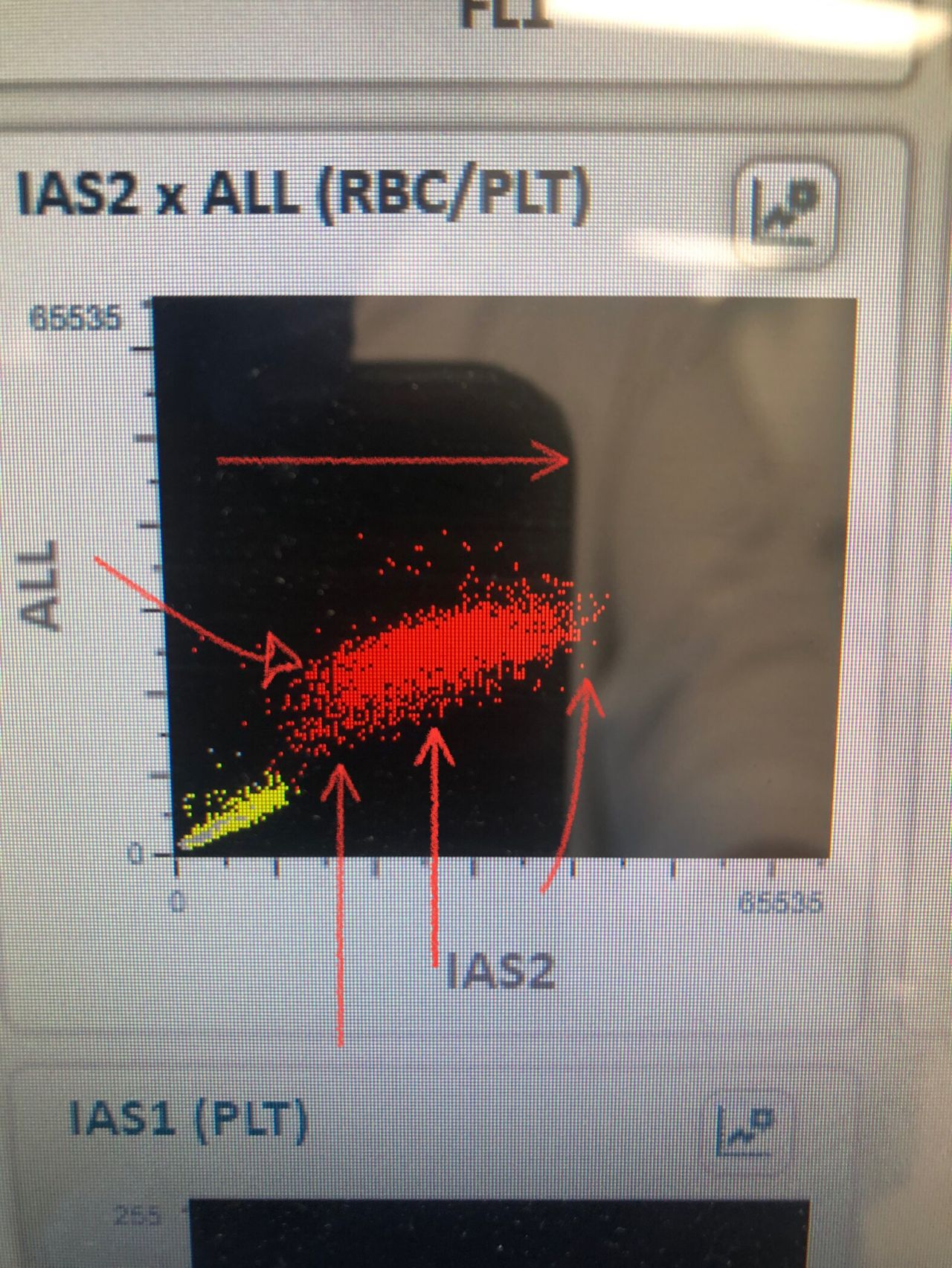
RBCs scatter shows 5 populations distributing from small to large in size confirming the high MCV really , also the RBC volume histogram shows the shift to right side , Macrocytosis
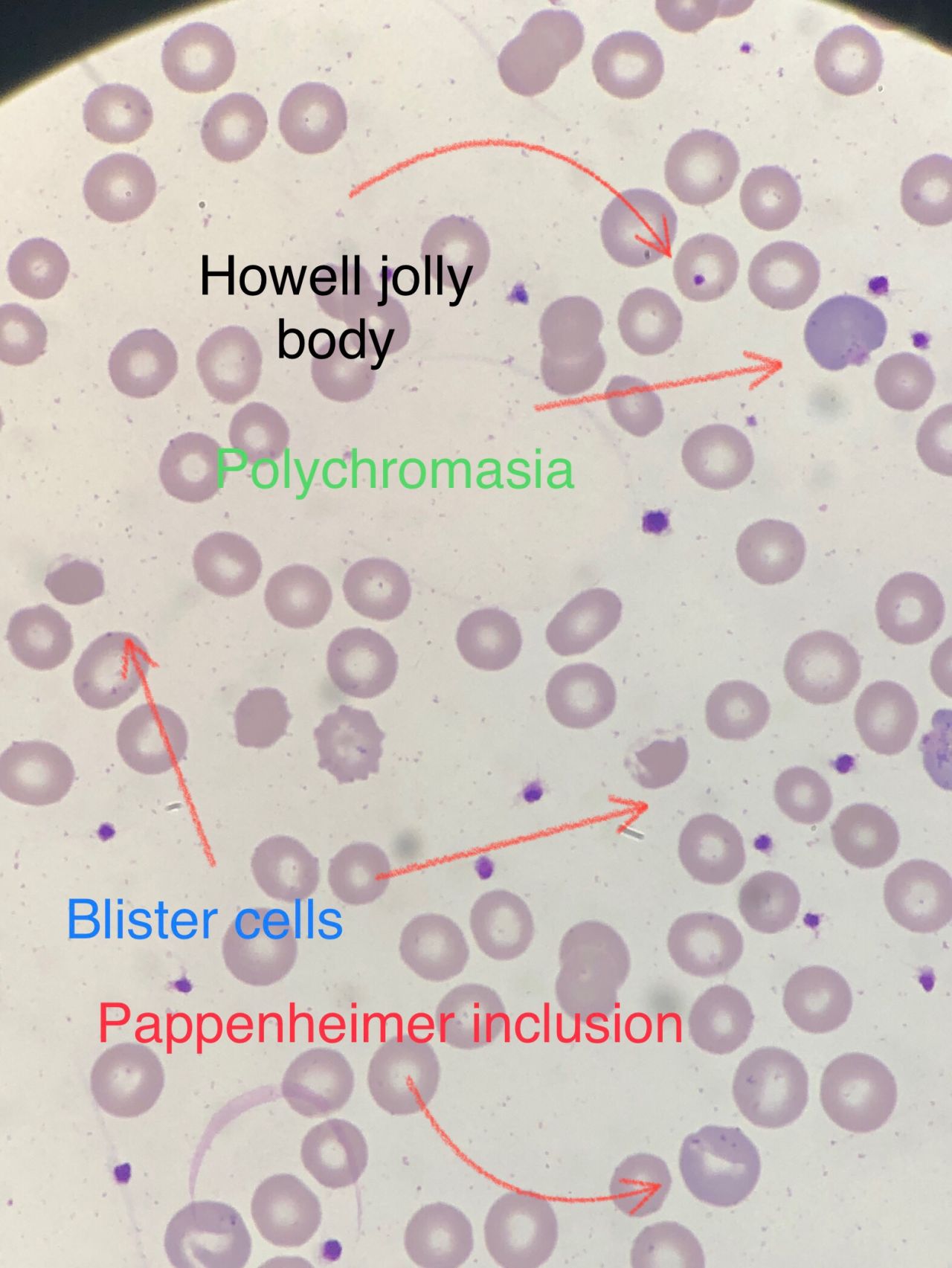
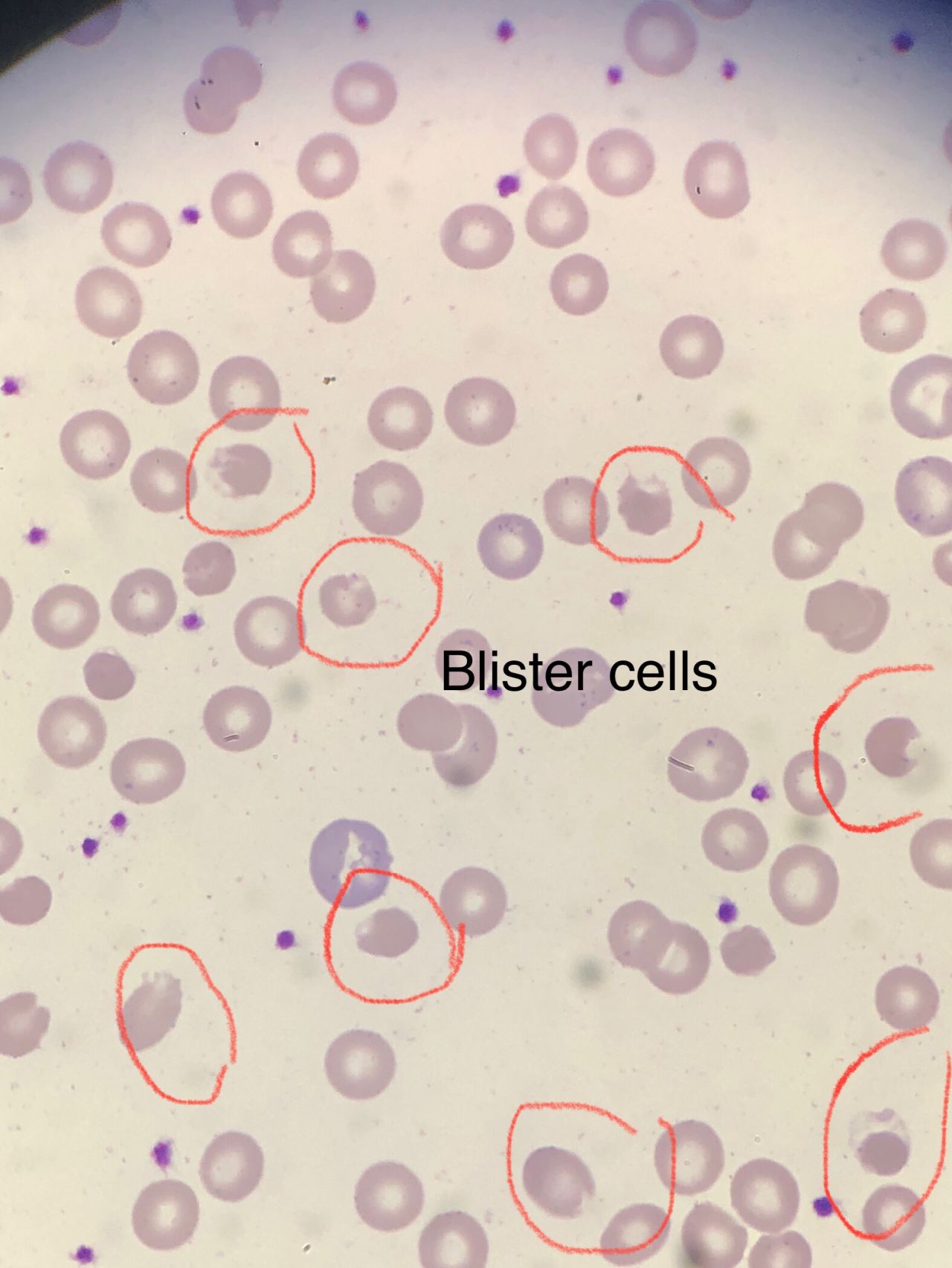
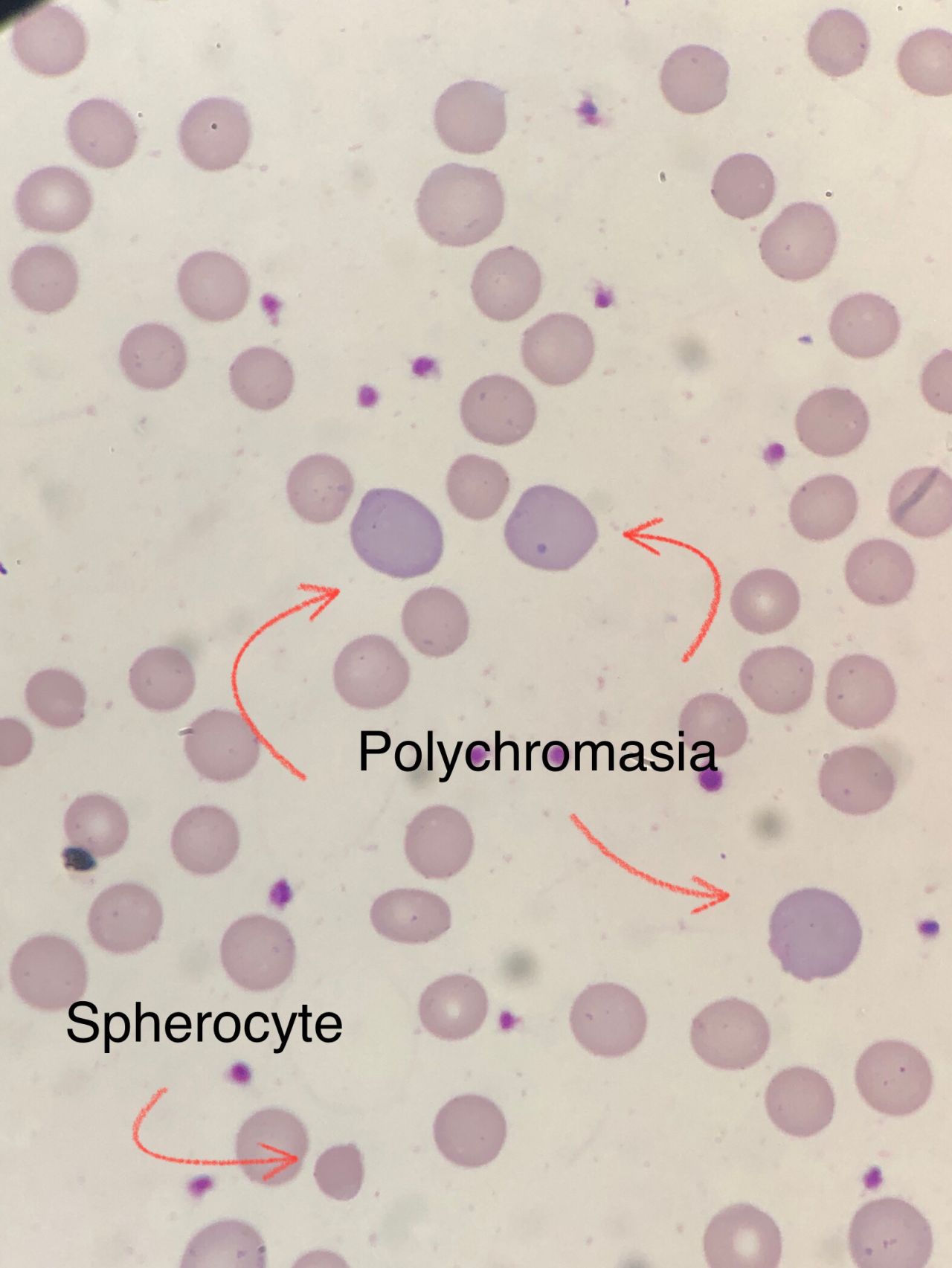
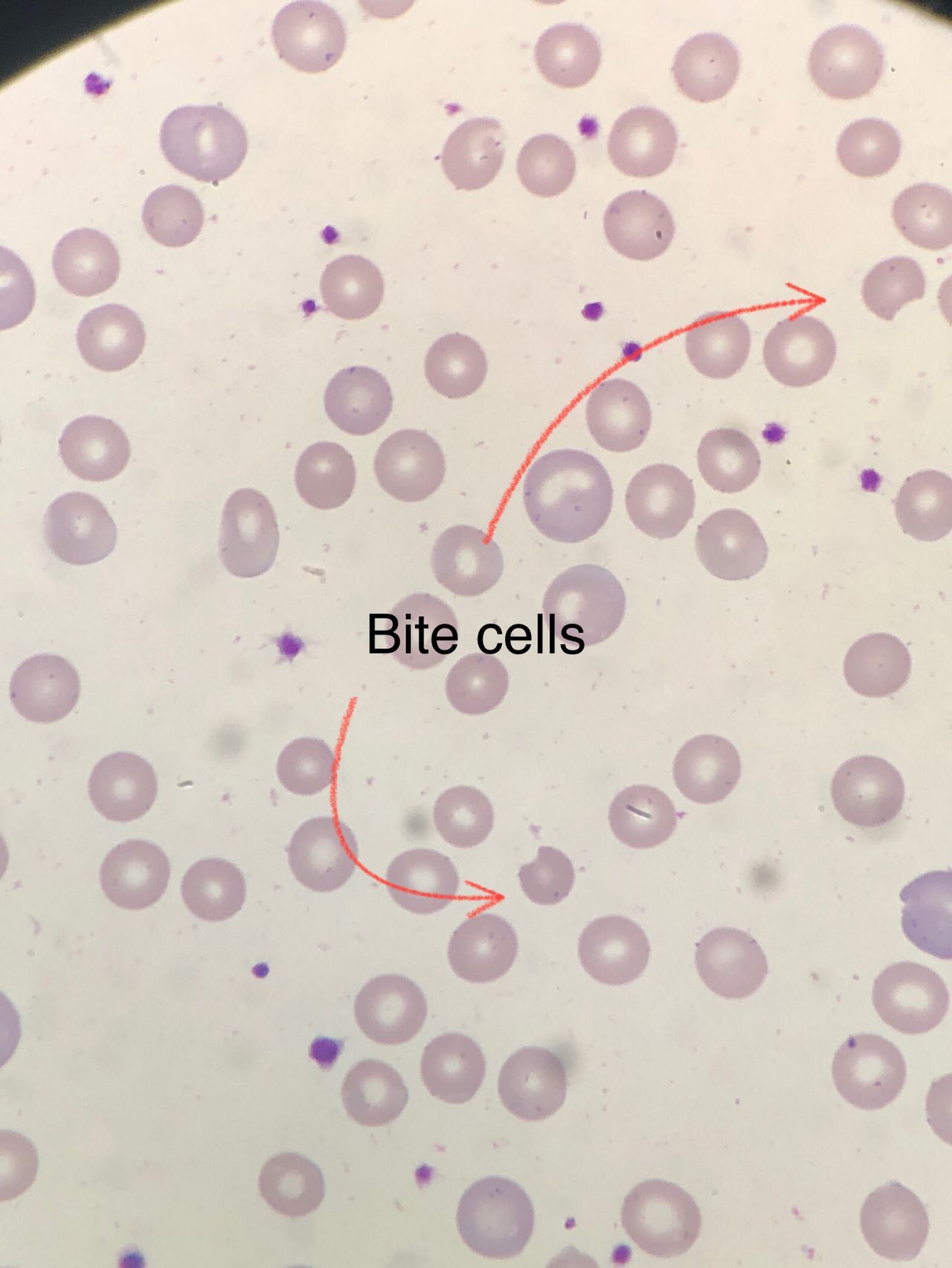
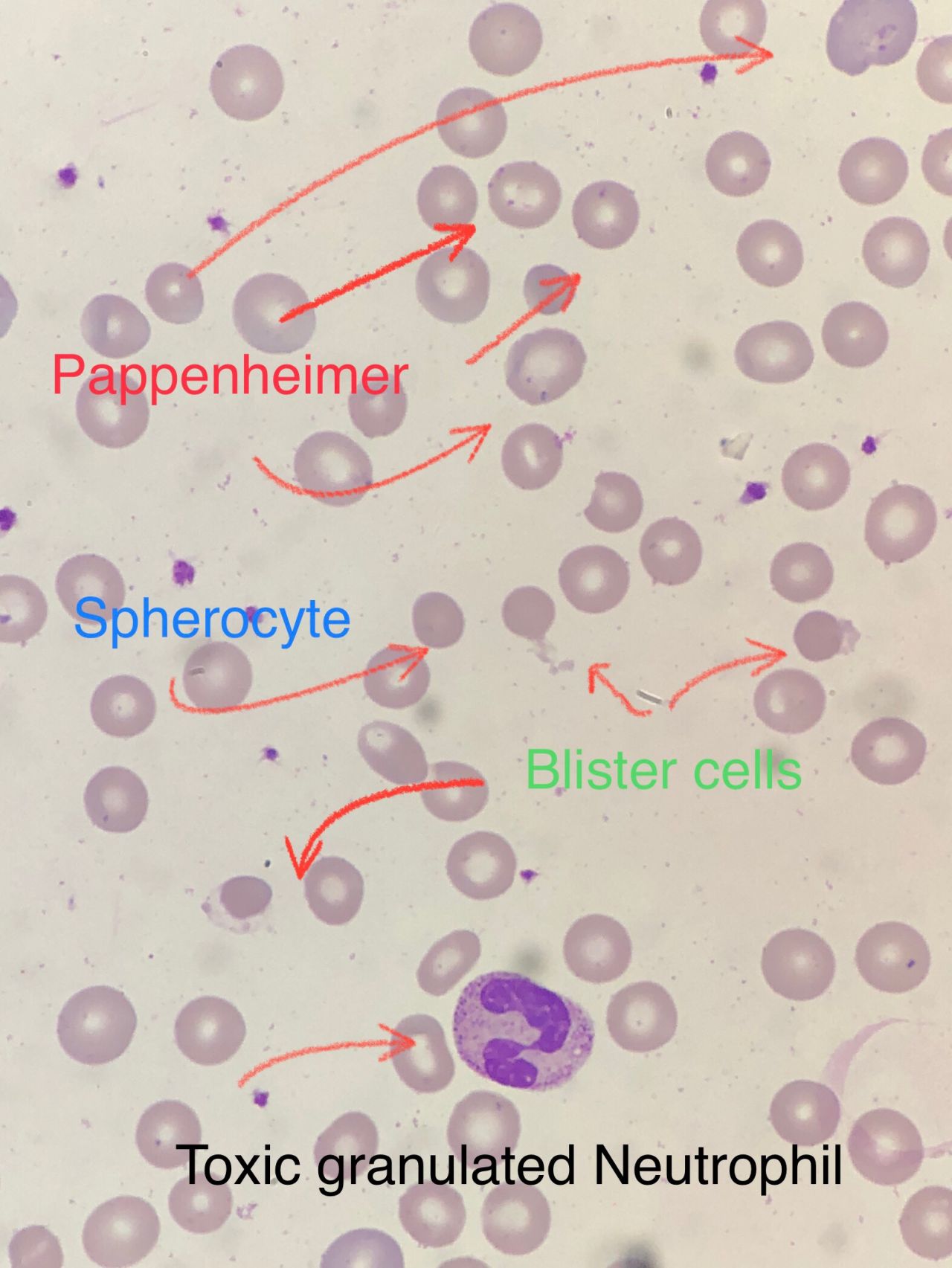
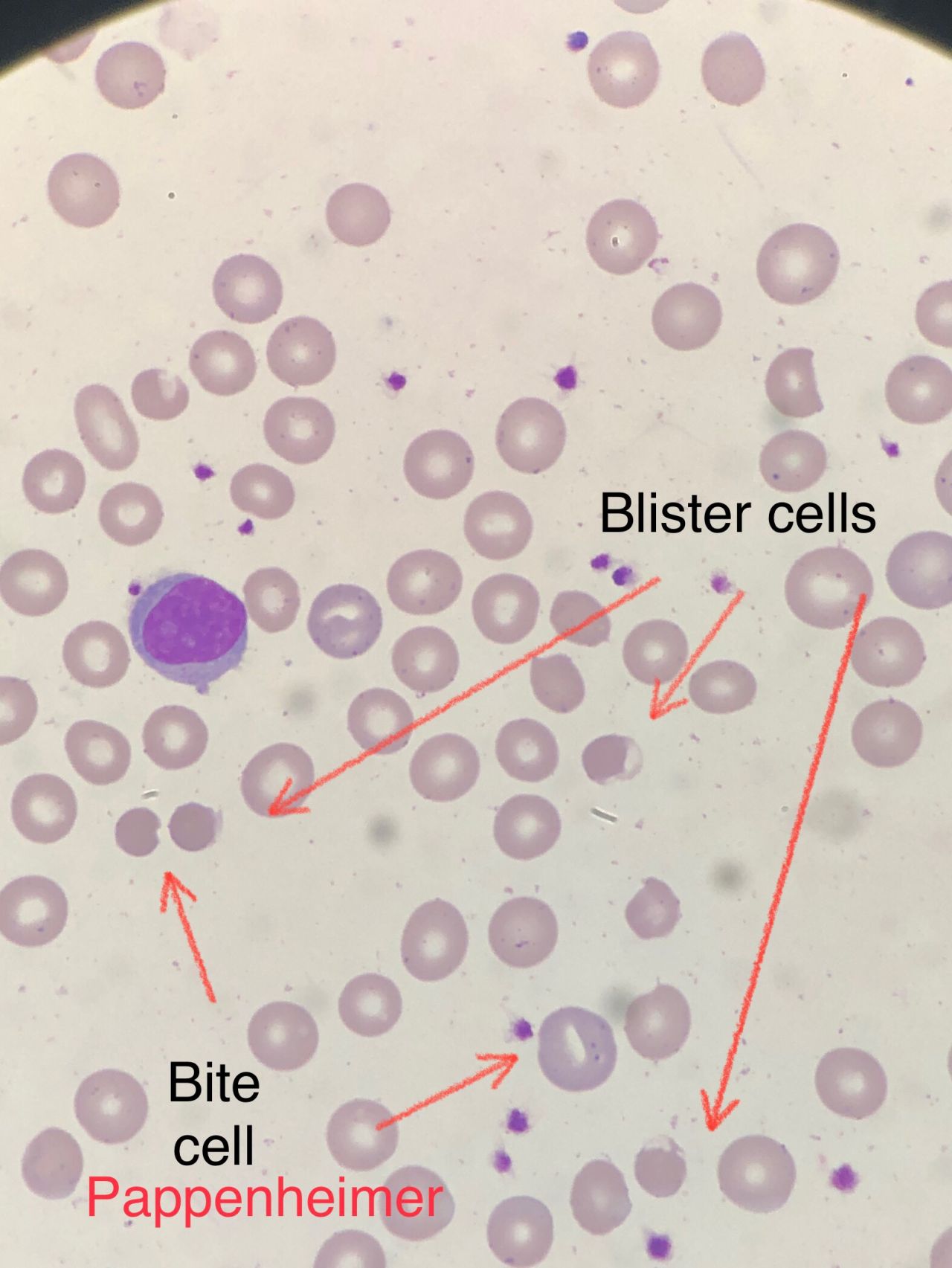
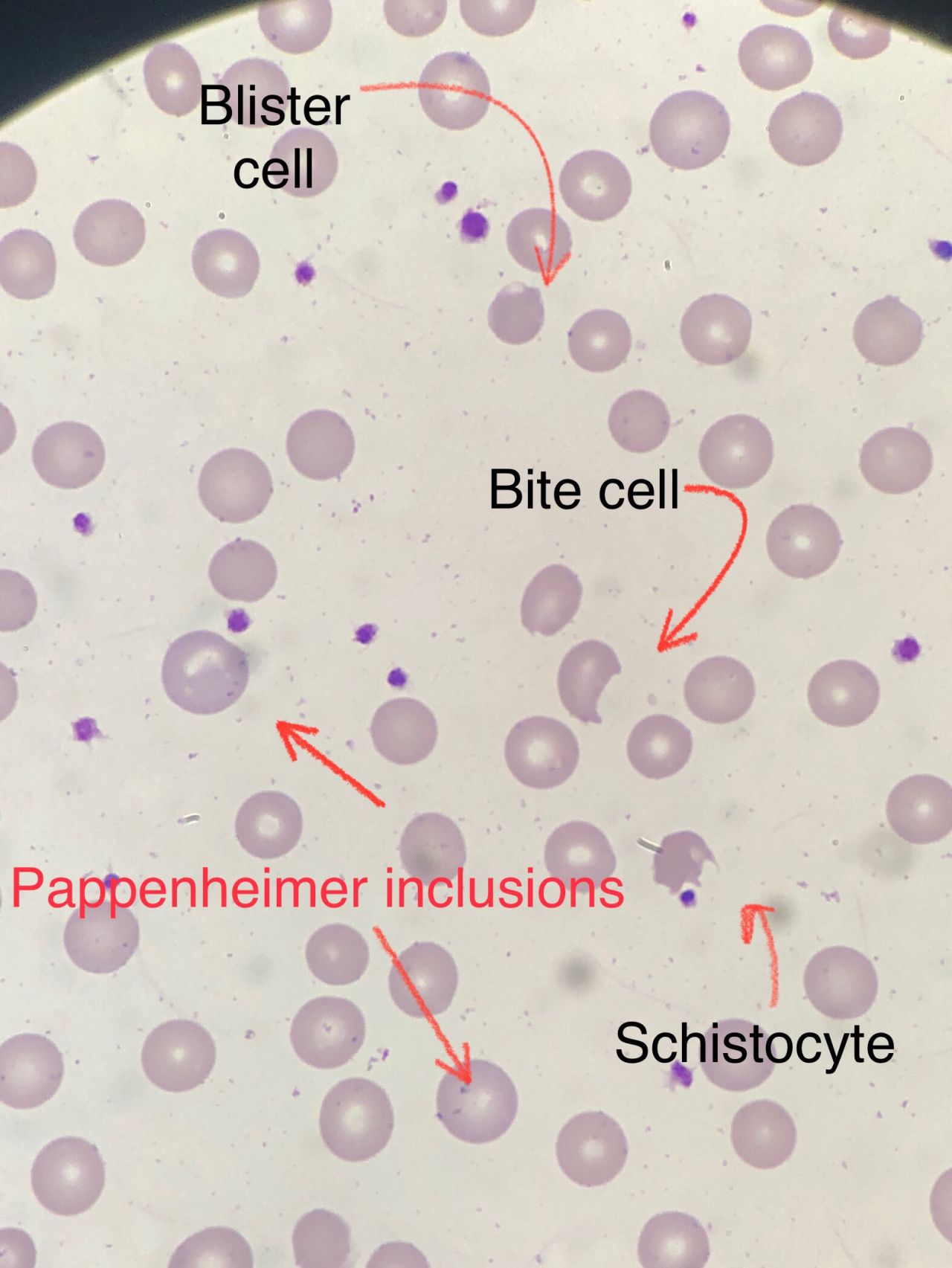
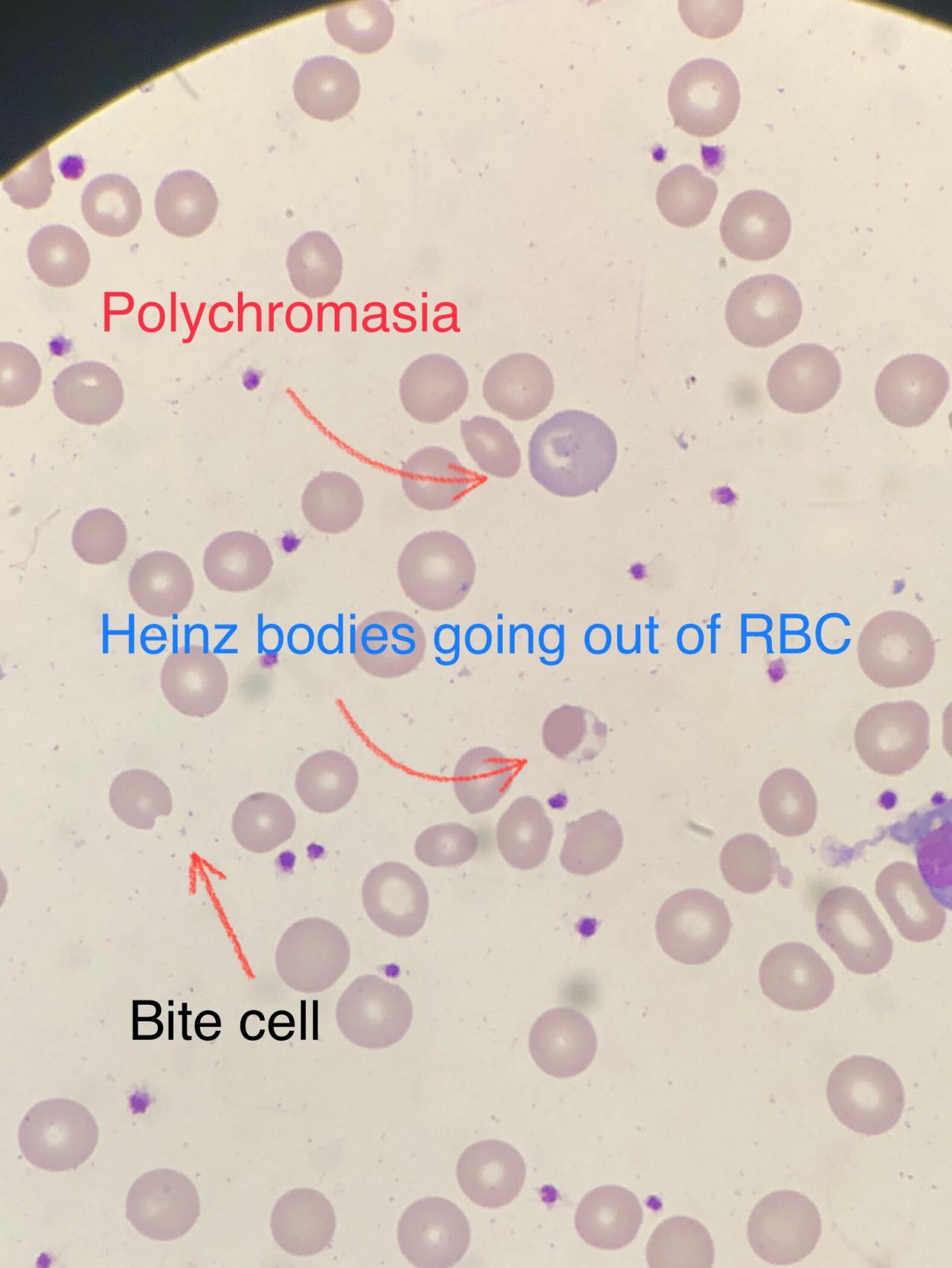
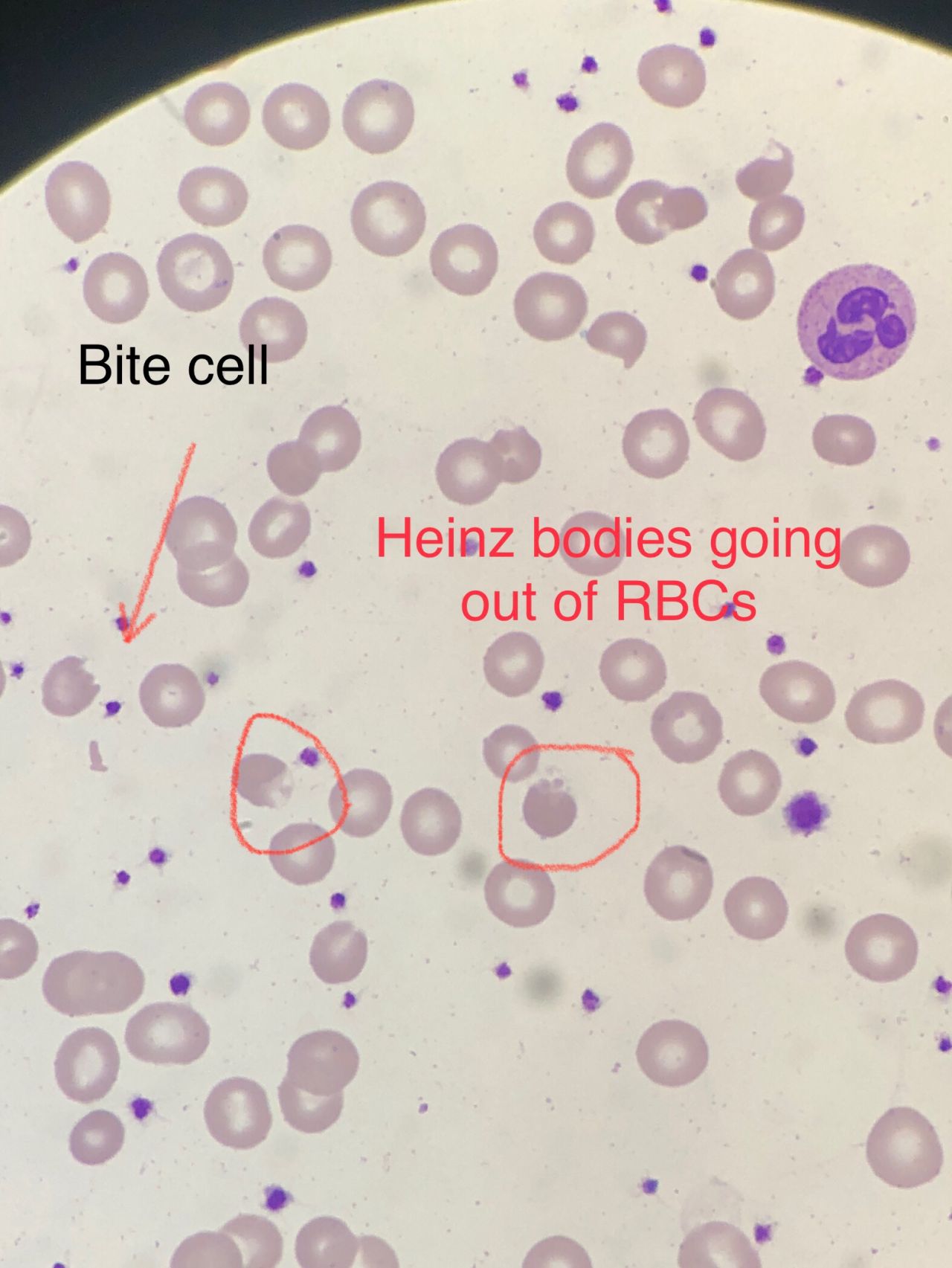
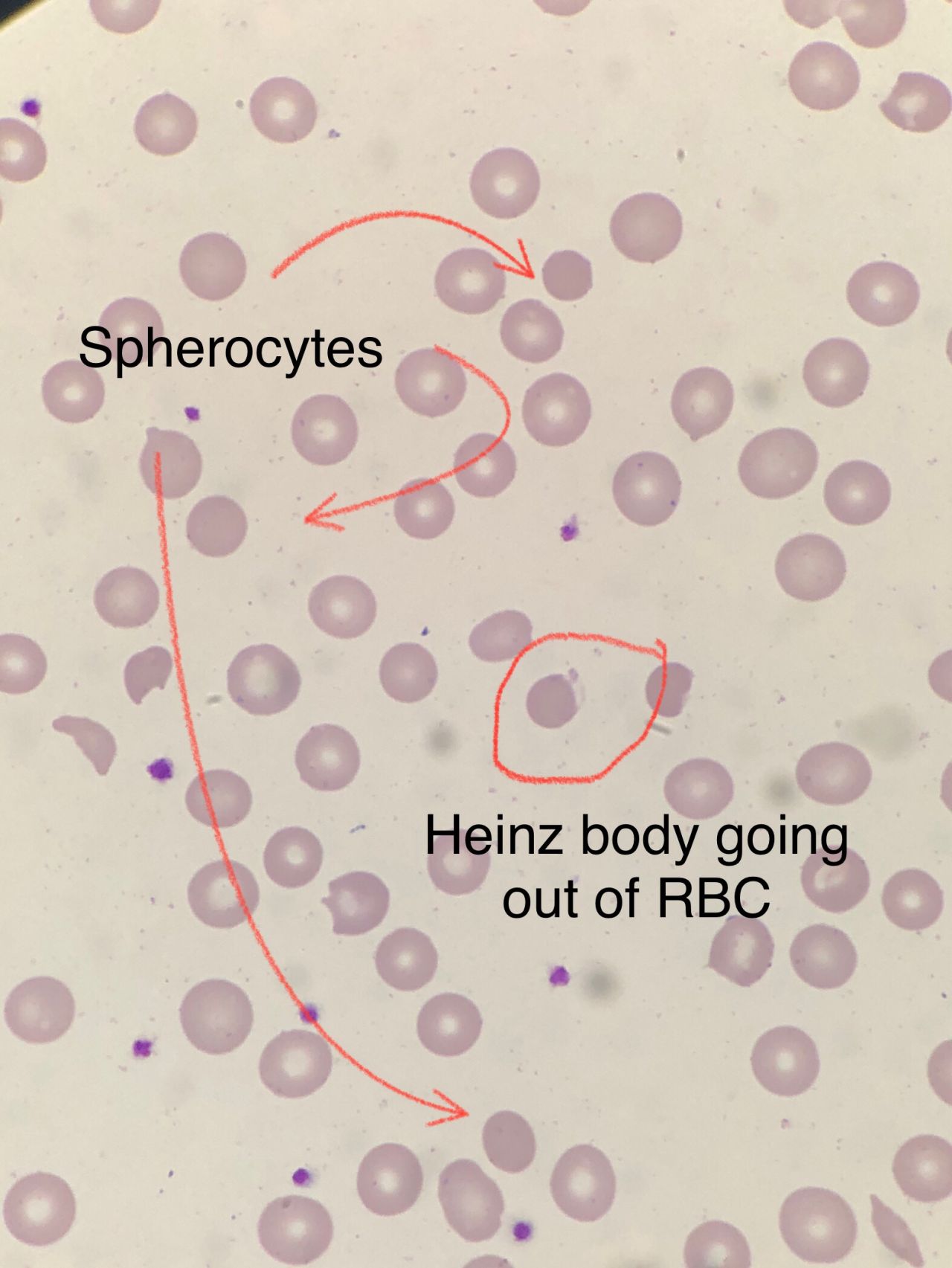
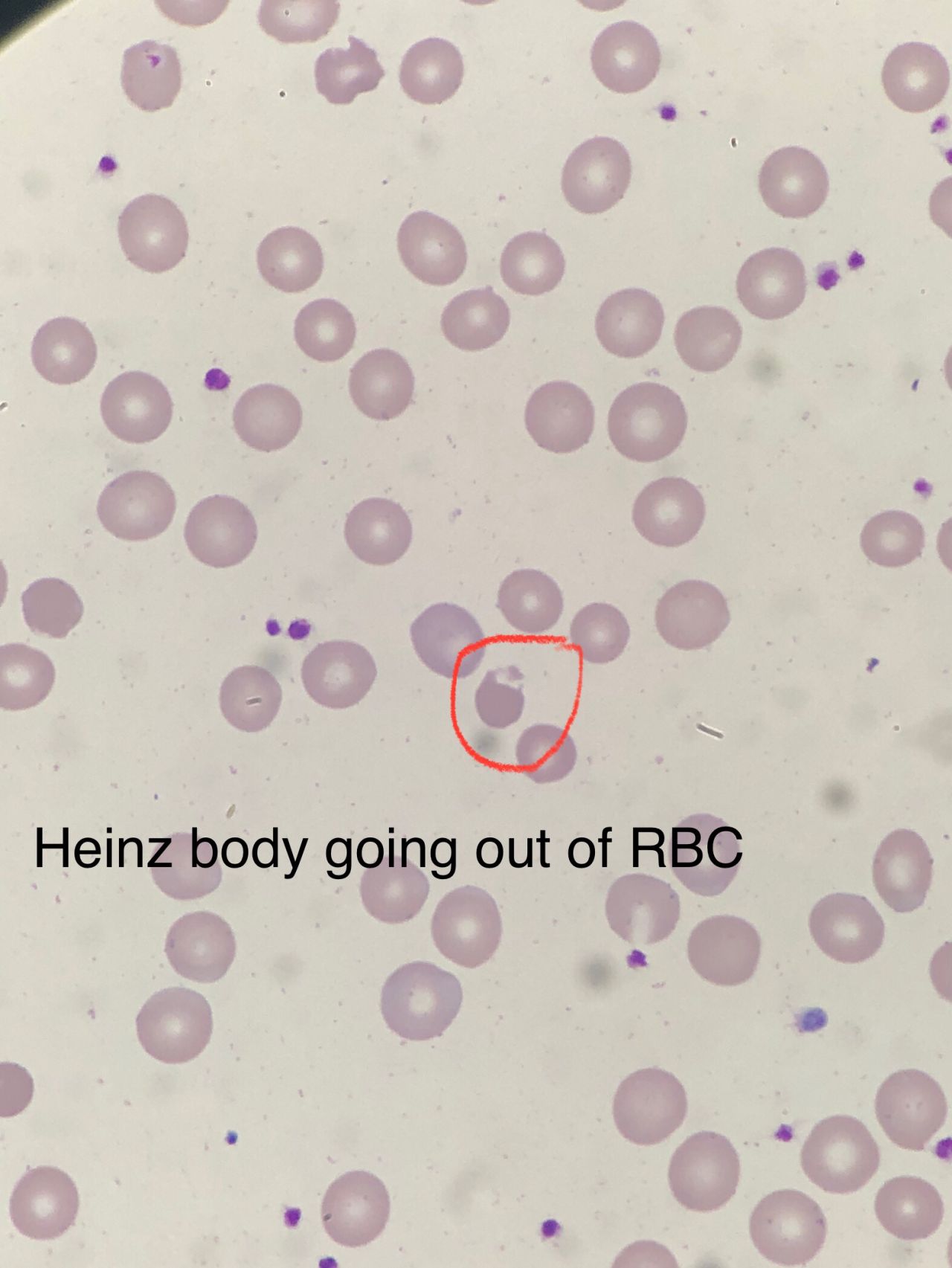
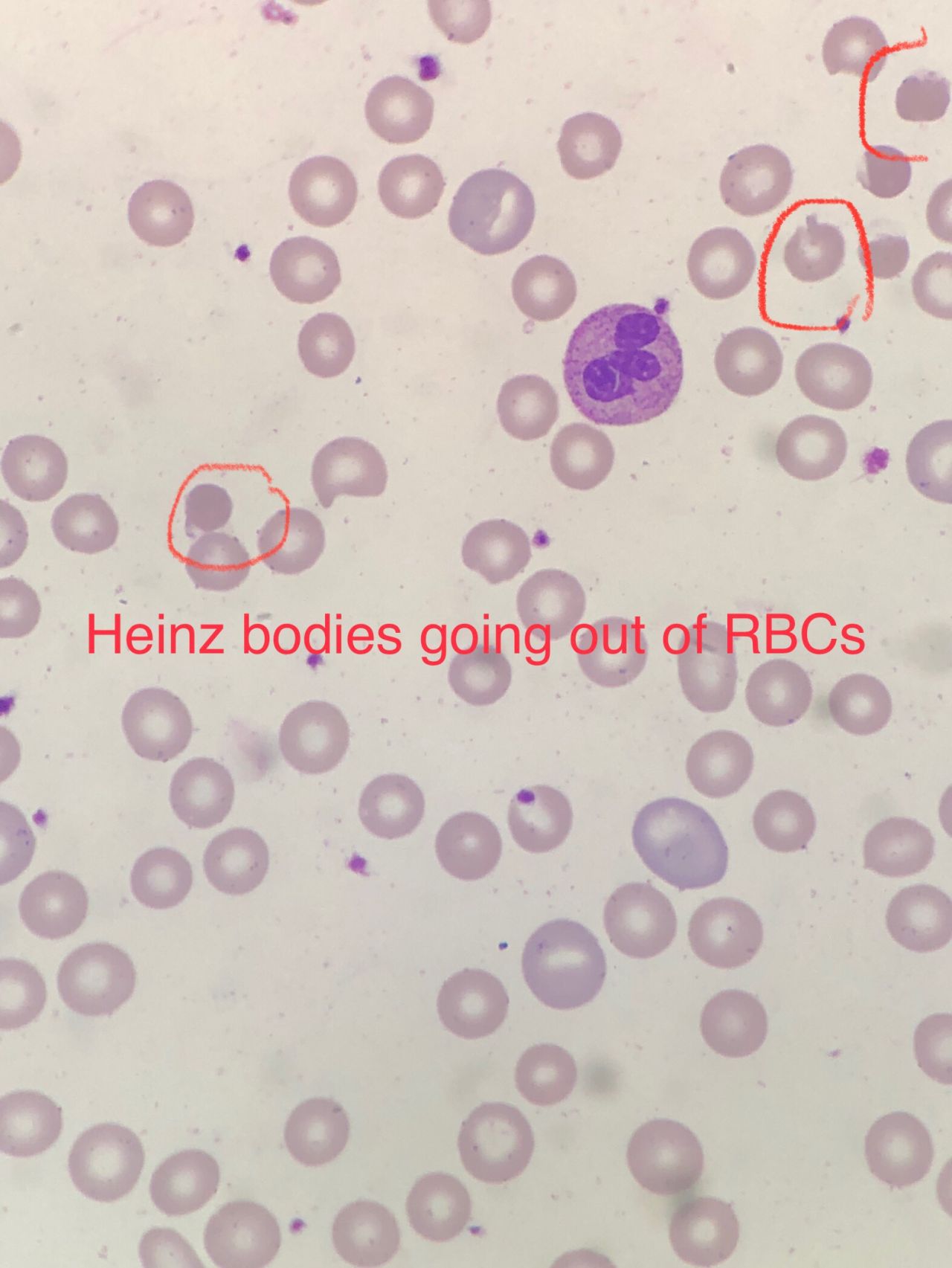
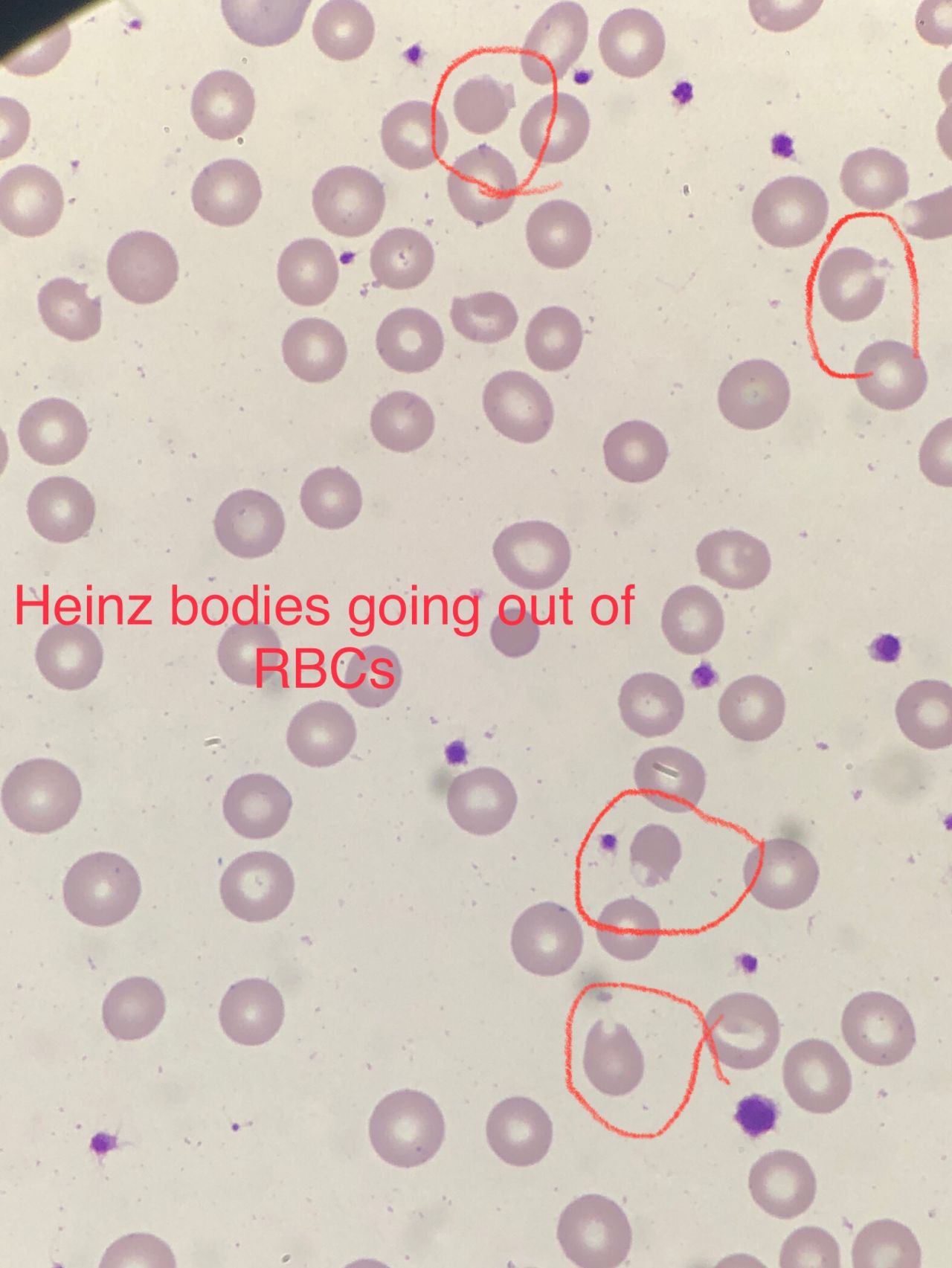
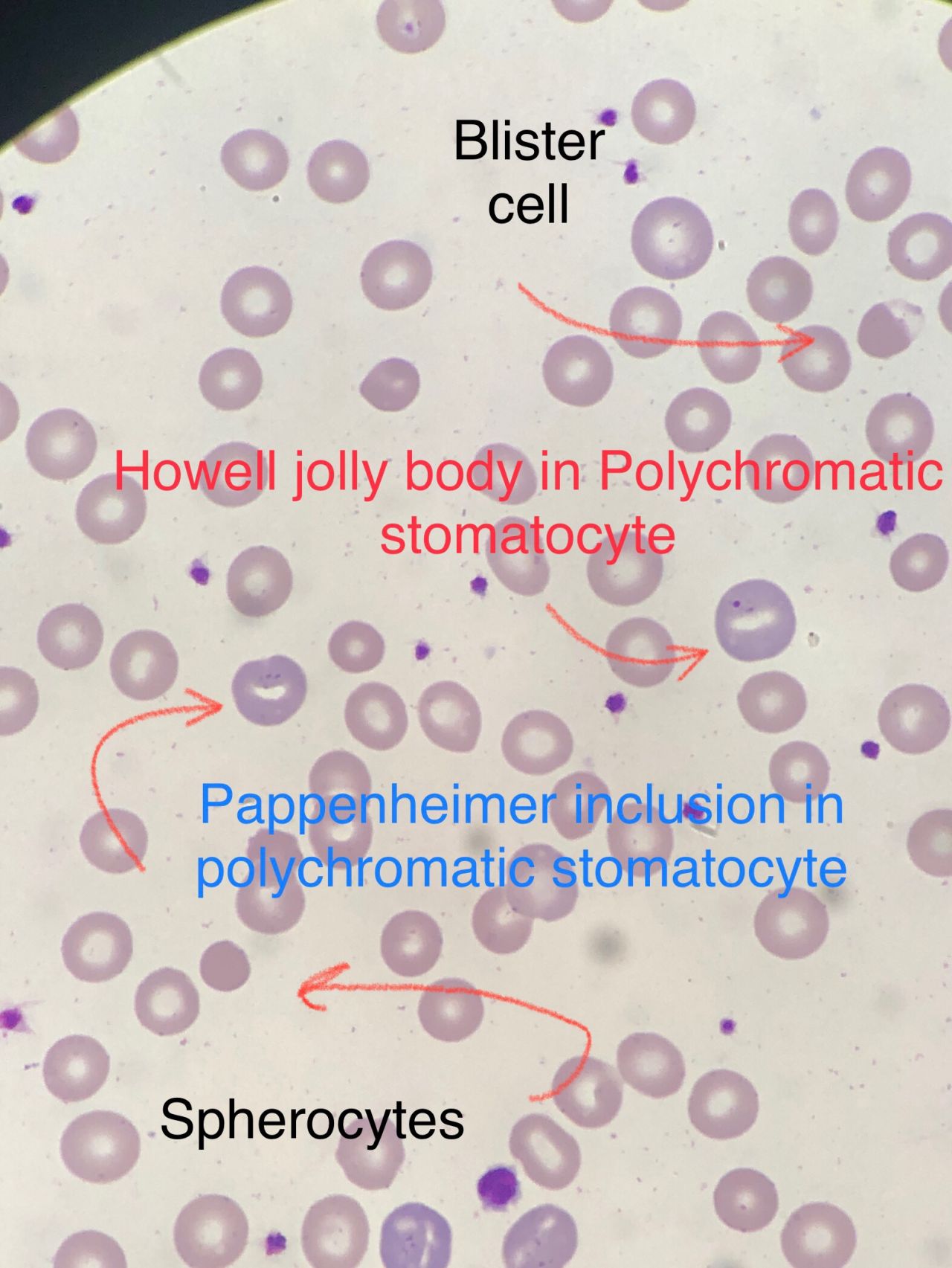
The slide really confirmed the hemolysis and high Retics he has . Polychromasia , Pappenheimer inclusions , Howell jolly bodies , Schistocytes , RBC fragments all seen . But then we have blister and bite cells , and amaizing some blisters are clear that Heinz bodies are going out of these RBCs , the leaving of Heinz bodies from inside will cause the shape of blister or bite cells when they go out and leave their place empty . So we did G6PD test and it was deficient even he is in hemolytic stage crisis . But the high MCV and as you can see Macrocytes and clear came from where ? Or from what ?
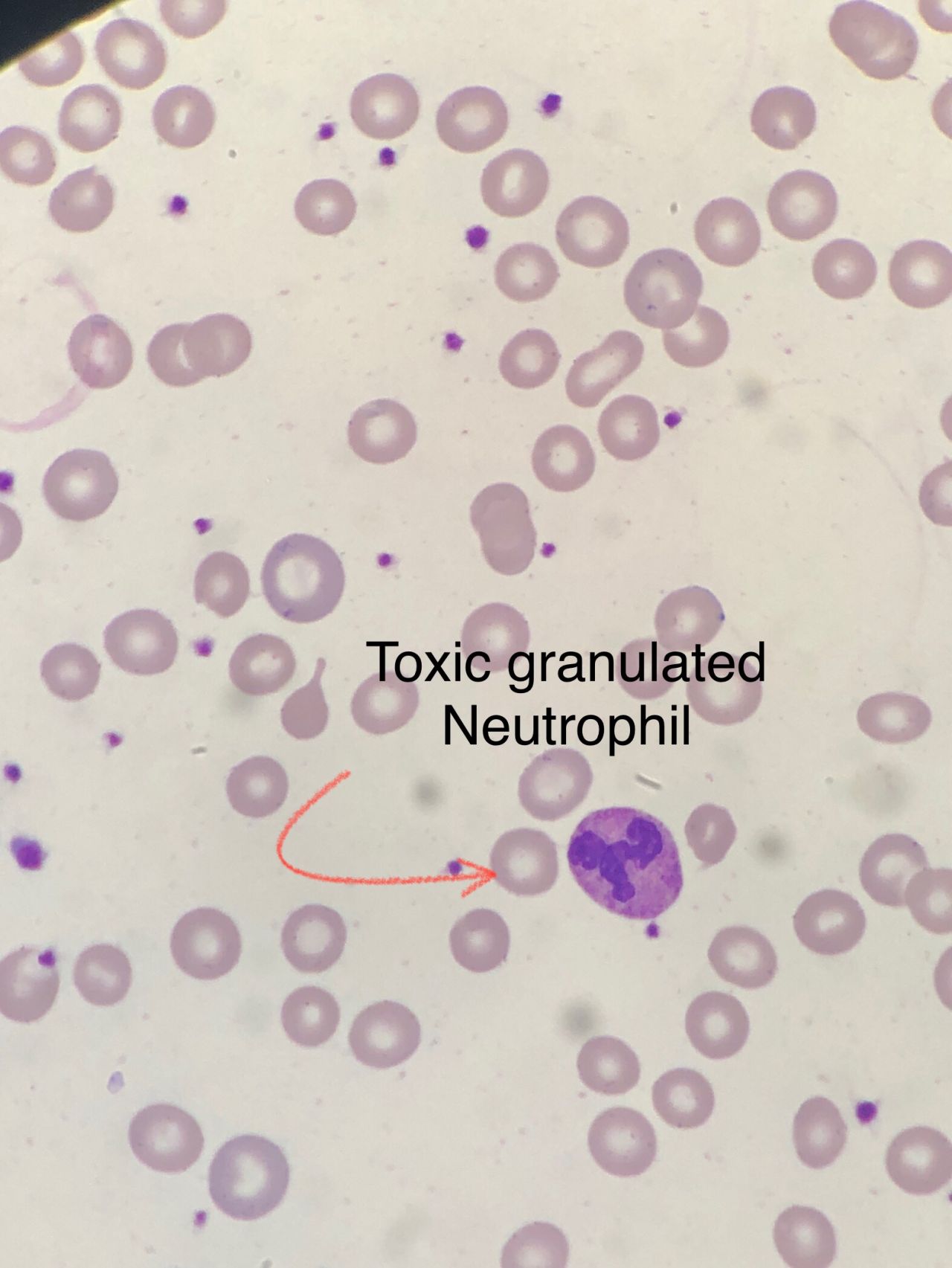
By checking his file in the history in the system I found that he has Vit.B12 deficiency and that was why he is following up in our hospital but no one knew he has G6PD also , even him self maybe . And as far we all know that G6PD patients don’t show any crisis after the age 12 years from food , so I think the trigger for the G6PD was from the treatment he is taking , he had infectious status and was under antibiotic treatment and that is clear from the toxic granulated Neutrophils . One of these medication was the trigger for this , and this was the strange combination of G6PD with Vit.B 12 deficiency
A G6PD crisis combined with Vitamin B12 deficiency presents a complex clinical picture involving two distinct causes of anemia: acute hemolytic anemia from the G6PD crisis and potential megaloblastic anemia (which can also involve hemolysis) from the B12 deficiency. Management requires identifying and removing the G6PD trigger, providing supportive care for the acute hemolysis, and initiating appropriate treatment for the B12 deficiency.
He was admitted directly from ER to have blood transfusion urgently then they will check his status , but at least now they know he has G6PD so he will not have crisis at all in the future inshaallah , he will be fine inshaallah and continue his treatment from the vit.B12 and be fine soon we hope , and God bless you all.”
 Badran: Our Case Contain Very Strange and Rare Combination of 2 Causes of Hemolytic Anemia 1")
Stay updated with Hemostasis Today.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-
Jul 9, 2026, 05:41Julieta Rosales: Management of Tandem Strokes – To Stent or Not to Stent?
-
Jul 8, 2026, 21:30Matthew Gouveia: How VNS-REHAB Is Transforming the Future of Stroke Rehabilitation
-
Jul 8, 2026, 21:22What Hundreds of Stroke Stories Have Taught Diana Kerr About Recovery and Resilience – Stroke Foundation
-
Jul 8, 2026, 19:50Heghine Khachatryan: Why the EHC Fully Supports the Lancet Commission on Women’s Hematological Health
-
Jul 8, 2026, 19:40Autoregulation Failure in SVD and Cognitive Impairment – International Journal of Stroke
-
Jul 8, 2026, 19:30Ahmed Mostafa: Why Antibodies Cause Organ Rejection
-
Jul 8, 2026, 19:28Erika Bocanegra: Witnessing 25 Years of Progress in Bleeding Disorders Care
-
Jul 8, 2026, 19:27Ahmadou Ouedraogo: Do You Know Your Blood Type?
-
Jul 8, 2026, 19:26Javed Anees: An Evidence-Based Clinical Guide to ESA Therapy