
Joseph R. Shaw: Beyond Predictable Pharmacokinetics in DOAC Therapy
Joseph R. Shaw, Director of Research+ Program at Ottawa Department of Medicine, EHJ-CVP Associate Editor at European Heart Journal, shared on LinkedIn about a recent article he and Jack Ansell co-authored, published in JTH, adding:
”In our Forum article published in JTH, A Light in the Dark—Reframing Direct Oral Anticoagulant Pharmacokinetics and Pharmacodynamics for Near-Patient Decision-Making, co-authored with Dr. Jack Ansell, we challenge a long-standing assumption in anticoagulation care: that DOACs have ‘predictable’ pharmacokinetics.
Over the past 15 years, ‘predictable PK’ has become a shorthand explanation for why fixed-dose DOAC therapy works well.
Fixed dosing is not the issue; the question is whether predictable pharmacokinetics is still the right explanation.
Increasingly, the evidence points elsewhere.
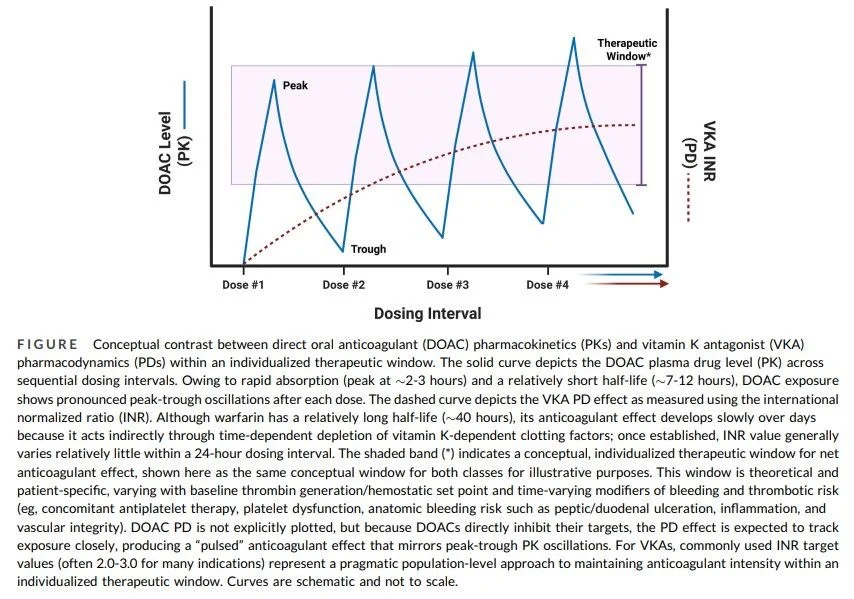
DOAC concentrations vary substantially between and within patients, raising a different question: are DOACs successful because their PK is truly predictable, or because their PD is more forgiving than that of VKAs?
Thrombin generation provides a unifying lens through which anticoagulant mechanism, PD profile, and clinical effect can be understood.
Across classes, a hierarchy emerges: broader, polypharmacologic agents can produce deeper suppression of endogenous thrombin potential, whereas selective inhibitors produce more constrained, class-specific PD effects.
In this framework, DOACs may work well for many patients not because drug levels are stable, but because selective single-factor inhibition produces downstream PD effects buffered across a wider exposure range than VKAs.
Antithrombotic benefit and acceptable hemostatic safety may persist across a broader concentration range, despite pronounced PK variability.
That relative PD predictability may improve safety on average, while limiting responsiveness under highly prothrombotic conditions.
The ‘predictable PK’ narrative has also had consequences.
It has reinforced the perception that DOAC levels have little clinical relevance, creating a false divide between the convenience of fixed dosing and the biology of coagulation and anticoagulant therapies.
Absence of evidence should not be confused with evidence of absence.
Levels matter because exposure, PD response, and clinical risk are connected; the unresolved question is when they matter most, how they should be measured, and how they should inform specific clinical decisions.
The goal is not routine monitoring for stable patients. It is targeted, time-sensitive decision support when a management decision is already required—the ‘clarity at the bedside’ problem.
Several DOAC-specific near-patient/point-of-care level tests are in development and may soon provide rapid, quantitative information when minutes matter.
To use these tools well, clinicians need an intuitive PK-PD framework for DOAC therapy, especially in major bleeding, urgent surgery, and thrombolysis for acute ischemic stroke.
I am grateful to my co-author, Dr. Jack Ansell, for the opportunity to write this article with him.”
Title: A light in the dark—reframing direct oral anticoagulant pharmacokinetics and pharmacodynamics for near-patient decision-making
Authors: Joseph R. Shaw, Jack Ansell

Stay updated on all scientific advances with Hemostasis Today.
{kind=link}
-
Jul 27, 2026, 03:34Wolfgang Miesbach: A Standout Talk by Jeffrey Weitz at ISTH 2026
-
Jul 26, 2026, 23:18Mohammadmahdi Sabahi: Proud to Share Our Complete Cushing’s Disease Research Collection
-
Jul 26, 2026, 22:59Mahmood Naseri: The Results of the 2nd Clinical Trial on AriClot Are Now Live in Burns Journal
-
Jul 26, 2026, 16:26Novi Yanti Sari: When MPNs Affect the Heart
-
Jul 26, 2026, 16:21Beyond Drugs: Can Museums Become a Medical Prescription?
-
Jul 26, 2026, 14:45Sarah Giorgia Grazia Giannone: An Exciting Chapter in Gene Therapy Research
-
Jul 26, 2026, 14:21Javed Anees: Cerebral Collateral Circulation in Acute Ischemic Stroke
-
Jul 26, 2026, 14:11André Picard։ Canadian Blood Supplies Drop Sharply, Urgent Donor Appeal Issued
-
Jul 26, 2026, 13:54Lorenzo Scalia: New Review Highlights Anticoagulant Strategies for Elderly Patients With Atrial Fibrillation