
David McIntosh Highlights Global Blood Shortages and Fresh vs Stored RBCs
David McIntosh, Founder and Chair at United Plasma Action, reposted from Archil Jaliashvili on LinkedIn:
“This is most interesting work.
However, I repost it with a warning.
What the World is desperately short of right now is a satisfactory supply of red cells – for uses where nothing else will do.
Fresh blood is better than older stored blood – especially for neonates.
We all know that. What’s really fatal is no blood at all.
In about 90% of all cases globally there IS NOT ENOUGH BLOOD.
Therefore, where choices have to be made; where priorities have to be set; the top priority has to be MORE BLOOD PLEASE.
Let’s not get distracted from that fact by anything … not by anything at all, until every blood bank in every hospital in the World has ample stocks.”
Archil Jaliashvili shared in Pharmaceutical & Medical Network: Biotech, Healthcare, Pharma, Devices, Science, Jobs, Events and News public group on LinkedIn:
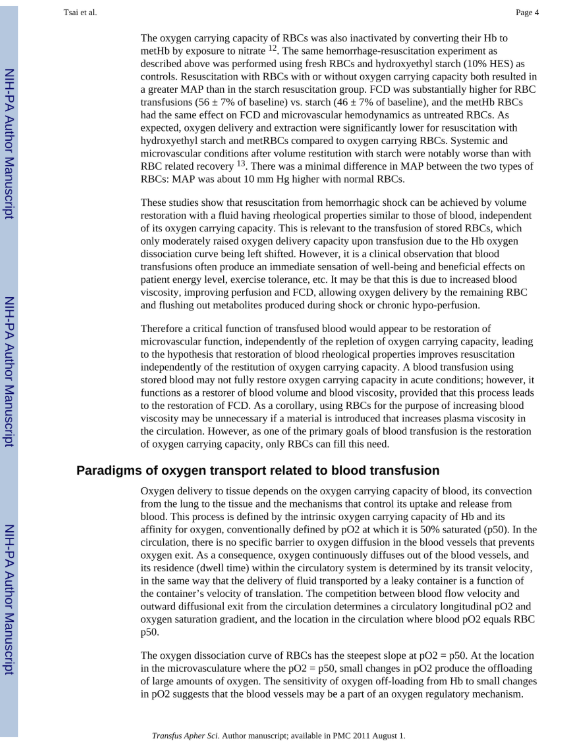
“What does a blood transfusion actually remedy?
In extreme hemodilution and hemorrhagic shock, focusing on the difference between fresh and stored RBCs.
Core Findings:
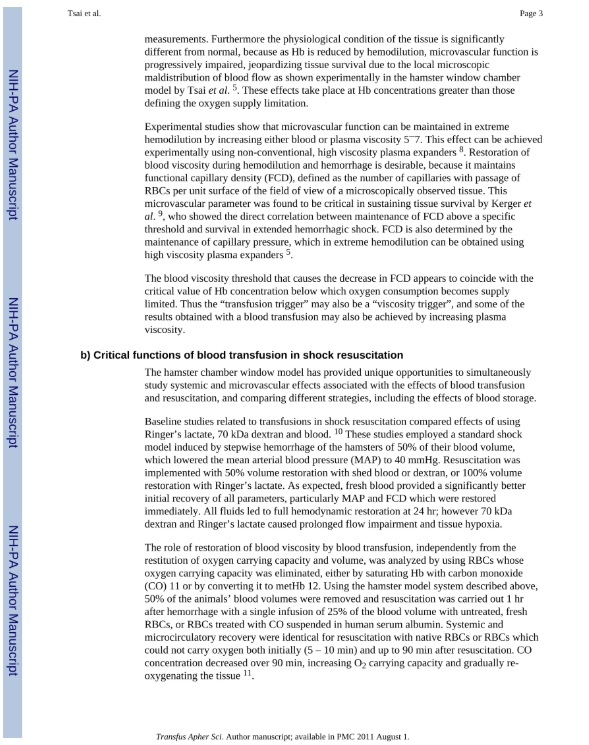
Clinically, transfusions are aimed at restoring oxygen-carrying capacity.
– Fresh RBC’ s restore both microvascular perfusion and oxygen capacity;
– Stored RBCs often restore viscosity but less effectively support microvascular perfusion and oxygenation.
Oxygen Affinity (p50)
– Stored RBCs lose 2,3-DPG.
RBC Storage Lesion
Progressive loss of deformability, ATP depletion, morphological changes, microvesicle shedding, increased aggregation, higher free hemoglobin.
These changes reduce FCD, impair O₂ delivery despite normal systemic parameters, and may cause vasoconstriction via NO scavenging.
NO Bioavailability
Hemolysis and free Hb from stored RBCs bind NO → vasoconstriction, reduced perfusion, and potential cardiovascular risk.
NO levels can recover in vivo, but the transient deficiency may be clinically important.
Experimental Conclusions
Fresh RBCs are consistently superior to stored RBCs in animal models — particularly for restoring microvascular perfusion and oxygenation.
The survival benefit may depend as much on restoring FCD as on oxygen capacity.
Clinical transfusion triggers based solely on hemoglobin may overlook perfusion deficits.
Why it matters – Oxygen Bridge: A Bridge to Recovery
BHOC – Biological Hemoglobin Oxygen Carrier.
-No Cross-Matching Required – Ready for immediate use in emergencies.
-High Oxygen-Carrying Efficiency and good perfusion.
-Immediate Restoration of Oxygenation – No need for factors like 2,3-DPG to function.
-Universal Complement to any cases where need efficient oxygenation.
Why it’s key: BHOC is not just a transfusion substitute — it’s an oxygen bridge, ensuring life-saving oxygen delivery in critical moments, from trauma to surgery, when every second counts.
Link to company.

Stay informed with Hemostasis Today.
{kind=link}
{kind=link}
{kind=link}
-
Jul 16, 2026, 20:25Ilham Benzidia: Leaving ISTH 2026 With New Ideas and New Collaborations
-
Jul 16, 2026, 20:23Eman Hassan: A Fantastic Platelets and Megakaryocytes Session at ISTH 2026
-
Jul 16, 2026, 20:22Sankara Nelson Noah II: Investigating the Temporal Dynamics of Platelet – Leukocyte Interactions in Early Sepsis
-
Jul 16, 2026, 20:20Joseph Pierre Aboumsallem: Paris Certainly Delivered This Week, and Not Just Because of the Heat
-
Jul 16, 2026, 19:53Louise St. Germain Bannon: The End of Congress, the Beginning of New Collaborations
-
Jul 16, 2026, 19:18Steve Humphreys: Learning From the Leading Experts at ISTH 2026
-
Jul 16, 2026, 19:02Kellie Machlus: Where Science Meets Friendship at ISTH 2026
-
Jul 16, 2026, 18:51Aaron Paul Kithcart: When Clinical Research Comes Together at ISTH 2026
-
Jul 16, 2026, 18:40Sara Buonomo: Predicting Relapse in Immune-Mediated TTP at ISTH 2026