
Chokri Ben Lamine: Hematology Pearls on Portal Vein Thrombosis
Chokri Ben Lamine, Adult Hematology and SCT Assistant Consultant at Oncology Center of Excellence at King Faisal Specialist Hospital and Research Center, shared a post on X:
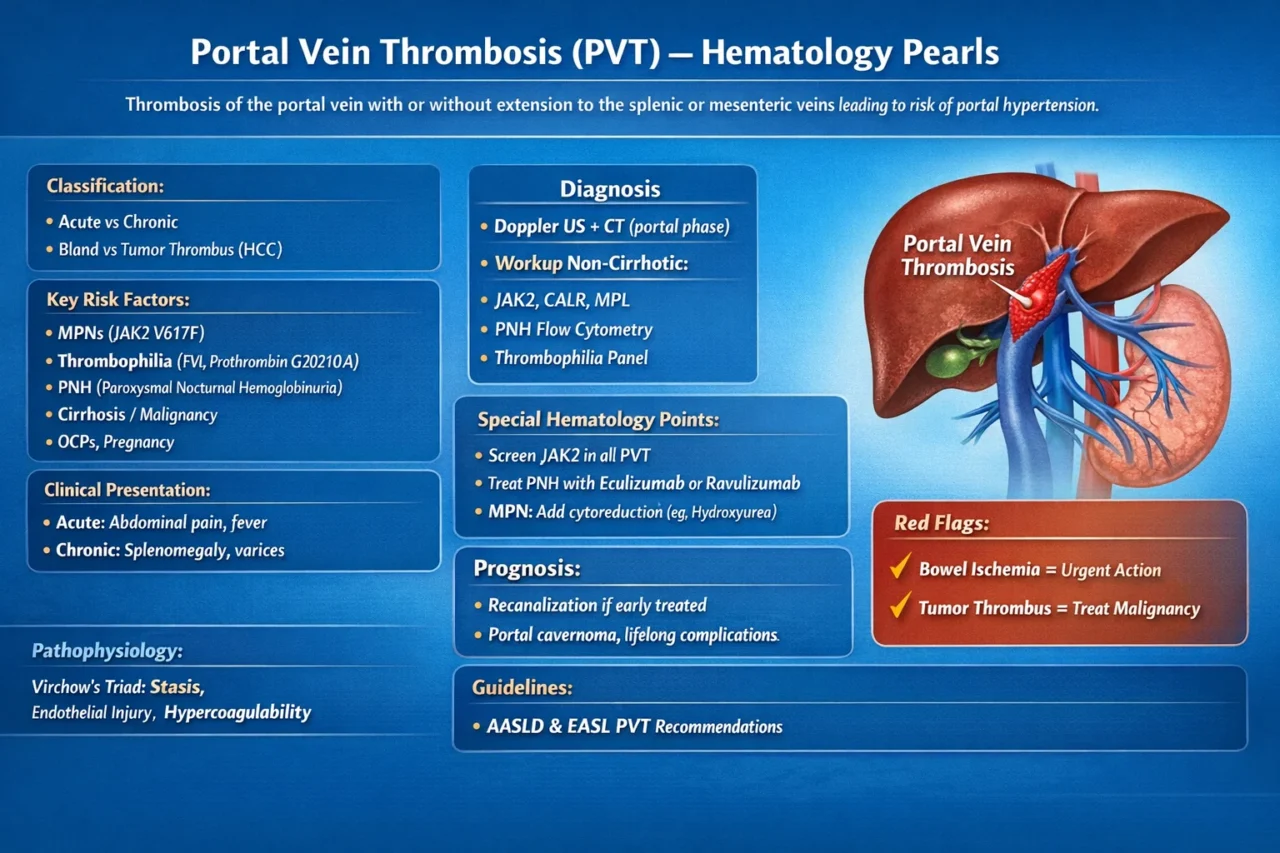
“Portal Vein Thrombosis (PVT) – Hematology Pearls
Thrombosis of the portal vein with or without extension to the splenic vein or superior mesenteric vein leading to risk of portal hypertension
Classification
- Acute vs chronic
- Bland vs tumor thrombus ( HCC)
Key Risk Factors:
- MPNs (especially JAK2 V617F positive) are the most common systemic cause
- Thrombophilia:
- Factor V Leiden
- Prothrombin G20210A mutation
- Decreased Protein C and Protein S
- Decreased Antithrombin
- PNH (always screen in unexplained PVT)
- Intra-abdominal infection/inflammation (appendicitis, pancreatitis)
- Cirrhosis / malignancy
- OCPs, pregnancy
Pathophysiology:
Virchow triad leads to portal flow stasis and endothelial injury, and hypercoagulability
Clinical Presentation:
Acute: abdominal pain, fever, nausea, increased lactate (if bowel ischemia).
Chronic: asymptomatic progressing to splenomegaly, varices, and thrombocytopenia.
Diagnosis:
- Doppler US is first line
- CT in the portal venous phase is the gold standard for assessing the extent of disease and for detecting bowel ischemia.
- Workup ALL non-cirrhotic:
- JAK2 positive or negative, CALR or MPL
- PNH flow cytometry
- Thrombophilia panel (selective, timing matters)
Red Flags
- Bowel ischemia leads to urgent anticoagulation and surgery
- Tumor thrombus leads to no anticoagulation alone (treat malignancy).
Management (Guideline-based):
- Anticoagulation is the cornerstone.
- LMWH changes to DOAC or VKA (individualized).
- Duration is three to six months or more.
- Indefinite if there is MPN or it is unprovoked.
Cirrhosis:
- Anticoag SAFE if no active bleeding (AASLD/EASL)
- Improves recanalization
Interventions:
- TIPS is indicated for refractory portal hypertension or disease progression.
- Thrombolysis is used in selected acute severe cases.
Monitoring:
- Imaging at three months shows recanalization.
- Platelets decreased, consider hypersplenism or MPN evolution.
Special Hematology Points:
- Always screen JAK2 in splanchnic thrombosis EVEN with normal CBC
- PNH clone is treated with Eculizumab or Ravulizumab.
- MPN-associated cases require adding cytoreduction, for example, with hydroxyurea.
Prognosis:
- Recanalization if early anticoag
- Chronic cases lead to portal cavernoma and lifelong complications.
Key Studies:
- AASLD 2020 guidance (vascular liver disorders)
- EASL 2016 PVT guidelines
- DeLeve LD et al., Hepatology.”
Stay updated with Hemostasis Today.
-
Jul 11, 2026, 19:56Louise St. Germain Bannon: A Fantastic Start to ISTH 2026 and the Future of Thrombosis Research
-
Jul 11, 2026, 19:38Lynn Kloeckner: Recognizing Kirsten Lacine’s Impact on the Stroke Survivor Journey
-
Jul 11, 2026, 19:19Rens De Groot: New Proteomic Evidence Reveals Early Hemolysis During ADAMTS13 Relapse in Immune TTP
-
Jul 11, 2026, 19:01Laurent Bertoletti: Honoring the Legacy of Guy Meyer and the INNOVTE Network at ISTH 2026
-
Jul 11, 2026, 18:53Pilar de la Rocha Mur: Why Trust Is the Most Valuable Currency in Clinical Research
-
Jul 11, 2026, 18:25First Pathogenic Deep-Intronic SERPINC1 Variant Identified in Hereditary Antithrombin Deficiency – JTH
-
Jul 11, 2026, 18:12Dianne E. van der Wal: A Thought-Provoking Discussion on Immunothrombosis at ISTH 2026
-
Jul 11, 2026, 16:07Louise St. Germain Bannon: Where Innovation Meets Collaboration at ISTH 2026
-
Jul 11, 2026, 15:22Cécile Denis: A Unique Opportunity for Emerging Hemostasis Leaders