
Deepali Derashri: Why Is Homocysteine a Silent Disruptor of a Healthy Pregnancy?
Deepali Derashri, Former Research Intern at Dr. B. Lal Clinical Laboratory, shared a post on LinkedIn:
“Homocysteine is not just a number on a lab report.
It can be a silent disruptor of a healthy pregnancy.
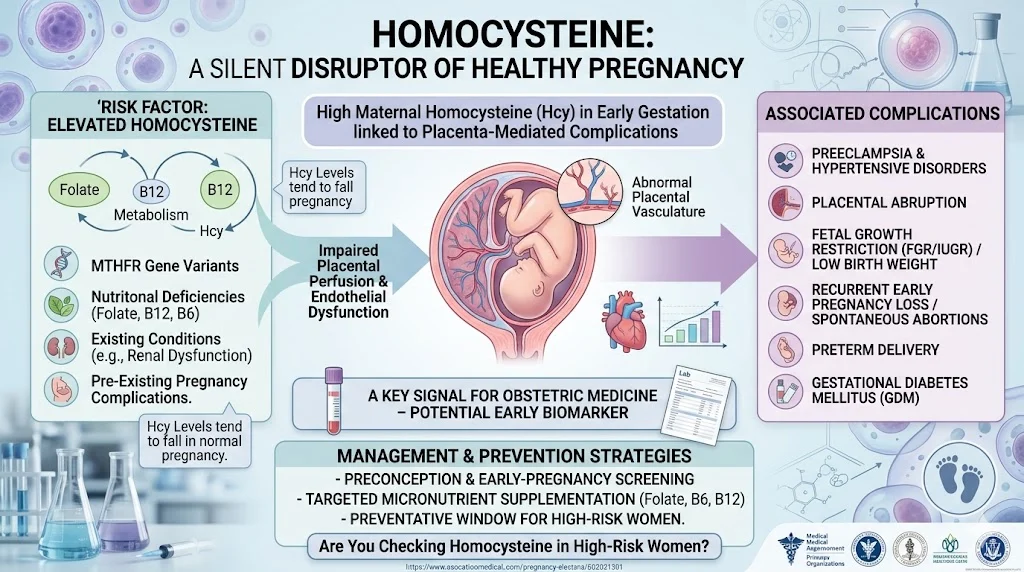
Emerging evidence shows that elevated maternal homocysteine (hyperhomocysteinemia) is linked with several placenta‑mediated complications, including:
- Preeclampsia and other hypertensive disorders of pregnancy
- Placental abruption
- Fetal growth restriction (FGR/IUGR) and low birth weight
- Recurrent early pregnancy loss and spontaneous abortions
- Higher risk of preterm delivery and, in some cohorts, gestational diabetes mellitus (GDM)
Physiologically, homocysteine levels tend to fall during a normal pregnancy due to hemodilution, increased glomerular filtration, and fetal uptake.
When levels remain high in early gestation, they may contribute to endothelial dysfunction and abnormal placental vasculature, setting the stage for impaired placental perfusion and downstream complications for both mother and baby.
Recent cohort and review data are particularly concerning: Women with raised homocysteine in the late first trimester show significantly higher rates of preeclampsia, abruption, fetal growth restriction and recurrent pregnancy loss compared to those with normal levels.
This positions maternal homocysteine as a potential early biomarker for ‘placenta‑mediated’ risk long before clinical symptoms appear.
The good news? Hyperhomocysteinemia is often modifiable.
Nutritional factors like folate, vitamin B6 and B12 status play a central role in homocysteine metabolism.
Genetic variants (for example in MTHFR) and comorbidities such as renal dysfunction or hypothyroidism can further elevate levels and may warrant closer monitoring.
Preconception and early‑pregnancy optimization of micronutrient status, alongside standard antenatal care, may help reduce risk in vulnerable women.
For clinicians, researchers and public health planners, this raises important questions:
- Should high‑risk women (history of preeclampsia, placental abruption, recurrent miscarriage, IUGR) be routinely screened for homocysteine before or early in pregnancy?
- Can early identification and targeted supplementation meaningfully improve maternal–fetal outcomes, especially in low‑ and middle‑income settings where nutritional deficiencies are common?
How do we integrate homocysteine into existing risk‑stratification models without over‑medicalising pregnancy?
As the evidence base grows, homocysteine is moving from a cardiovascular risk marker to a significant signal in obstetric medicine. Strengthening awareness among obstetricians, family physicians, fertility specialists and policymakers could open up a valuable window for prevention – not just treatment – of pregnancy complications.
If you work in obstetrics, fertility, nutrition or public health:
Are you already checking homocysteine in high‑risk women?
Conversations on this under‑used marker and how we can leverage it to protect maternal and fetal health.”
Stay updated on all scientific advances with Hemostasis Today.
-
Jun 24, 2026, 09:29Advancing Women’s Health Through Collaboration with Jean Hailes for Women’s Health – Stroke Foundation
-
Jun 24, 2026, 09:18The Lasting Immunological Footprint of VITT – JTH
-
Jun 24, 2026, 09:09Umberto Pensato: Dedicated Funding Pathways for Stroke Research in Italy
-
Jun 24, 2026, 09:00Danny Gaskin: BBTS 2026 and the Evolving Role of Transfusion in Maternity Care
-
Jun 24, 2026, 07:46Wolfgang Miesbach: WFH’s First AAV Gene Therapy Chapter Marks a New Era in Hemophilia Care
-
Jun 24, 2026, 06:42Deepthi Krishna: World Blood Donor Day 2026 Celebrations at Rela Hospital
-
Jun 24, 2026, 03:36Ana Pedrero Gil: A New Approach to Post-Tonsillectomy Hemorrhage
-
Jun 24, 2026, 02:59Melissa Hollo: Making Early Anemia Detection the Standard of Care
-
Jun 24, 2026, 02:51Bruno Pougault: The Thin Line Between Bleeding and Clotting