

Jan Sloves: Iliac Vein Compression – Why Position Matters More Than We Think
Jan Sloves, President and Consultant at Vascular Imaging Professionals LLC, shared a post on LinkedIn about a recent article by Nicos Labropoulos et al., published in European Journal of Vascular and Endovascular Surgery:
“Iliac Vein Compression: Why Position Matters More Than We Think
We’re all seeing more referrals for ‘May-Thurner’ or ‘iliac vein compression’ in young women with pelvic venous symptoms.
What this new EJVES 2026 duplex paper by Nicos Labropoulos and colleagues drive home is that a lot of those ‘stenoses’ are not fixed lesions – they’re positional.
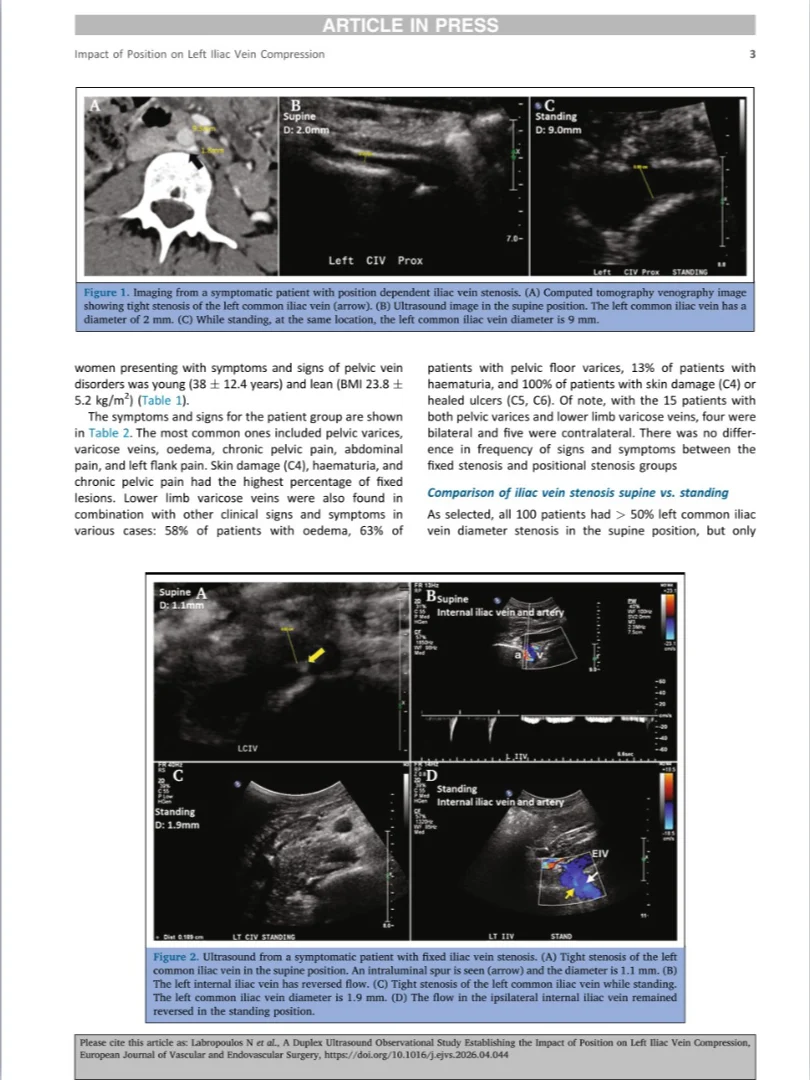
In this cohort of 100 symptomatic women, every single patient had more than 50% LCIV stenosis in the supine position.
Yet when they were scanned standing, only about one‑third still had more than 50% narrowing.
Two‑thirds essentially ‘opened up’ when upright.
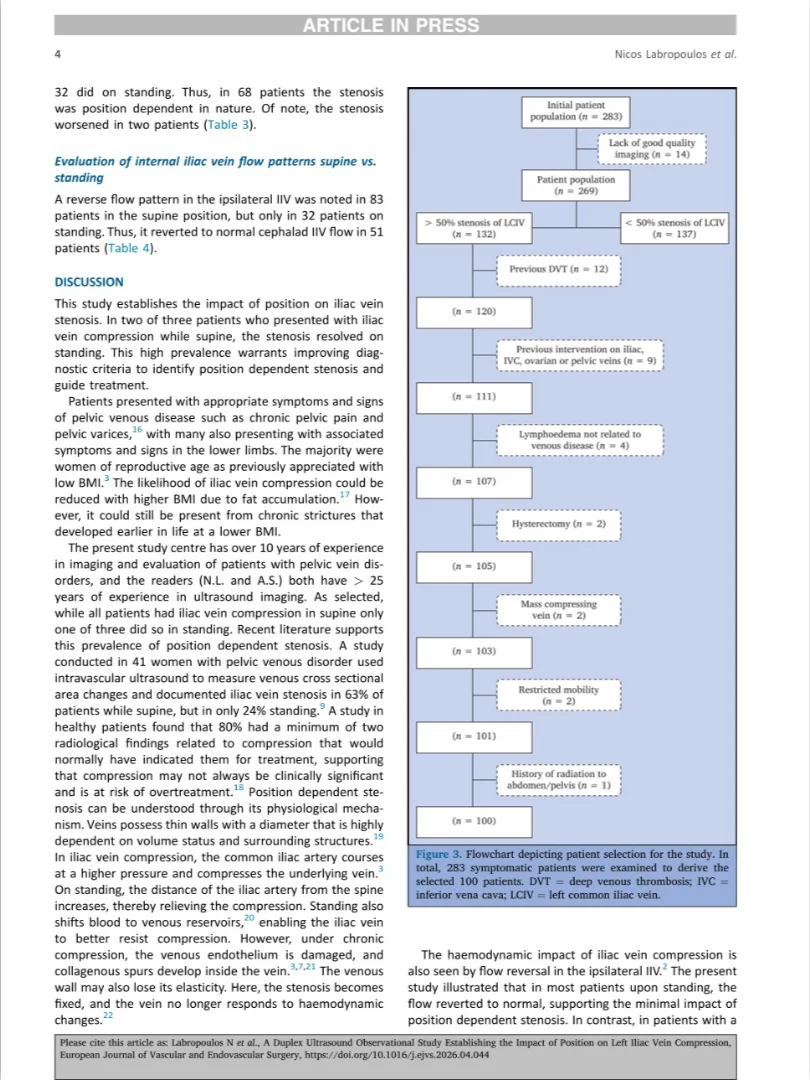
Their ipsilateral internal iliac vein flow did the same thing: 83% had flow reversal supine, but that dropped to 32% when standing as flow reverted cephalad.
Clinically, fixed and positional groups looked the same. Same pelvic pain, same pelvic varices, same lower extremity findings. In other words, anatomy alone did not tell you who had a truly haemodynamically relevant lesion.
This has big implications for how we scan and how we treat.
If you only image supine, you will over‑call “significant” stenosis and some of those patients will end up with stents for what is essentially a physiologic, posture‑dependent compression.
My take‑home: for pelvic venous disorder patients, iliac vein evaluation should not be a supine‑only study.
We should be routinely documenting LCIV calibre and IIV flow supine and standing and clearly labeling lesions as fixed vs positional in our reports.
And crucially, non‑thrombotic iliac vein lesions should not be stented based on axial imaging alone, without positional duplex or IVUS‑based functional assessment.
That one simple shift can help us better triage who truly needs an iliac vein intervention – and who doesn’t.
Subscribe to the only newsletter built for vascular pros.”
Title: A Duplex Ultrasound Observational Study Establishing the Impact of Position on Left Iliac Vein Compression
Authors: Nicos Labropoulos, Ashna Raiker, Alisha Raiker, Adriano Souza, Antonios Gasparis

Other articles featuring Jan Sloves on Hemostasis Today.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-
Jul 26, 2026, 23:18Mohammadmahdi Sabahi: Proud to Share Our Complete Cushing’s Disease Research Collection
-
Jul 26, 2026, 22:59Mahmood Naseri: The Results of the 2nd Clinical Trial on AriClot Are Now Live in Burns Journal
-
Jul 26, 2026, 16:26Novi Yanti Sari: When MPNs Affect the Heart
-
Jul 26, 2026, 16:21Beyond Drugs: Can Museums Become a Medical Prescription?
-
Jul 26, 2026, 14:45Sarah Giorgia Grazia Giannone: An Exciting Chapter in Gene Therapy Research
-
Jul 26, 2026, 14:21Javed Anees: Cerebral Collateral Circulation in Acute Ischemic Stroke
-
Jul 26, 2026, 14:11André Picard։ Canadian Blood Supplies Drop Sharply, Urgent Donor Appeal Issued
-
Jul 26, 2026, 13:54Lorenzo Scalia: New Review Highlights Anticoagulant Strategies for Elderly Patients With Atrial Fibrillation
-
Jul 26, 2026, 13:32Ahmed Kotb: A Practical Guide to Von Willebrand Disease