

Carlos Henrique Del Carlo: HFpEF and Iron Deficiency – Why Treating the Mitochondrial Engine Matters More Than We Thought?
Carlos Henrique Del Carlo, Collaborating Professor at University of São Paulo Medical School (FMUSP), Attending Physician at Heart Institute (InCor–HCFMUSP), shared on LinkedIn:
”HFpEF and Iron Deficiency: Why Treating the Mitochondrial Engine Matters More Than We Thought
HFpEF fatigue is not just hemodynamic – it is about cellular energetics.
We often describe HFpEF as a systemic inflammatory syndrome. But how does this inflammation translate into exercise intolerance?
One key link is frequently overlooked: iron deficiency (ID).
In heart failure, iron deficiency reflects impaired cellular metabolism and reduced oxygen utilization – not just low hemoglobin.
Relying solely on Hb means missing a substantial proportion of patients.
Why does iron deficiency matter in HFpEF?
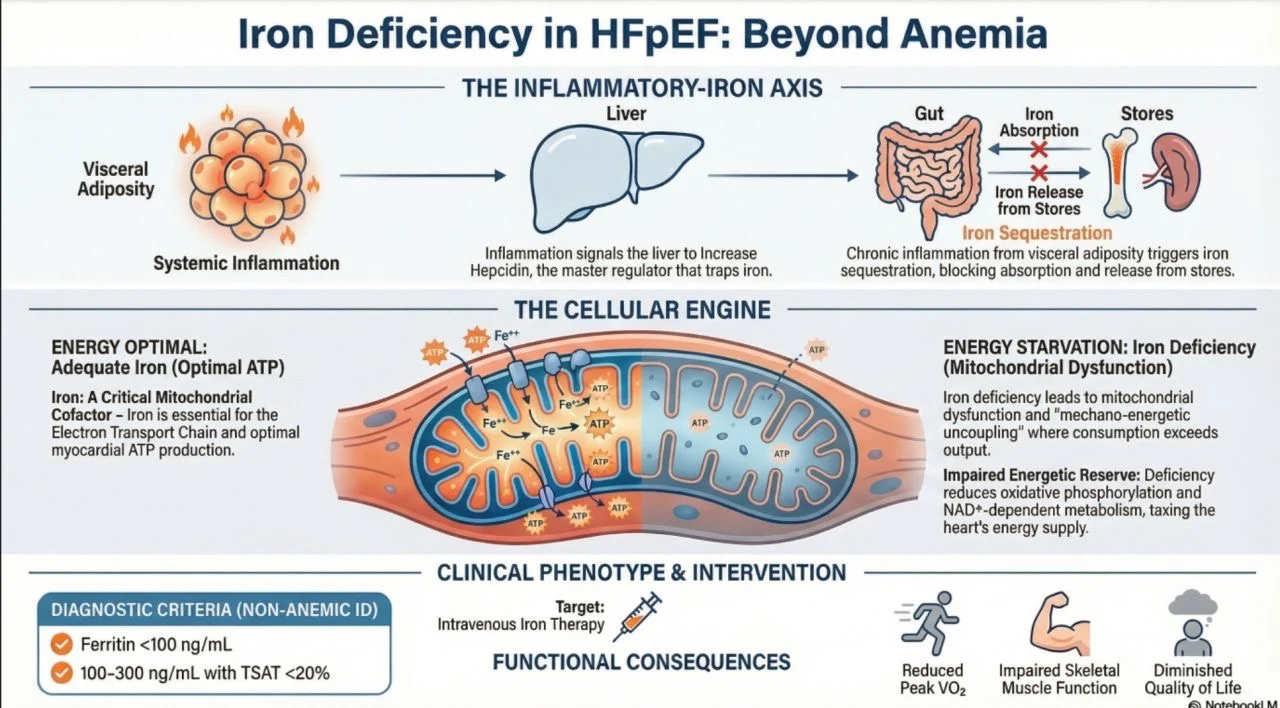
- The Inflammatory Block: Chronic low-grade inflammation – driven by visceral adiposity – increases hepcidin levels. This hormone effectively sequesters iron, making it unavailable for the heart and skeletal muscles.
- Mitochondrial Failure: Iron is a key cofactor for the mitochondrial respiratory chain. Without it, the ‘engines’ of the cardiomyocytes fail, leading to impaired peak VO2 and significant functional limitation.
- Beyond Anemia: Roughly 50% of HFpEF patients suffer from ID, yet many are not anemic. If we only screen for Hemoglobin, we miss the diagnosis in a large portion of this population.
The Clinical Challenge:
Recent evidence reinforces that addressing the metabolic substrate is as vital as managing congestion.
Intravenous iron has shown consistent improvement in exercise capacity (6MWT) and quality of life – even when hard endpoints like hospitalization are still being debated.
Diagnosis is simple, but we need to look beyond hemoglobin:
The traditional ferritin-based definition (<100 ng/mL, or 100–300 ng/mL with TSAT <20%) may not reliably identify patients who benefit from iron therapy.
Increasingly, TSAT <20% is considered a more evidence-based marker of clinically relevant iron deficiency.
If we only check hemoglobin, we miss the diagnosis.
The paradigm shift
- Iron deficiency in HFpEF is not a hematologic problem.
- It is a bioenergetic failure at the mitochondrial level.
Clinical perspective – Emerging evidence suggests:
- Intravenous iron – improves functional capacity and quality of life
- Oral iron – ineffective in HF (due to hepcidin-mediated absorption blockade)
- We are no longer just treating congestion. We are targeting the metabolic substrate of the disease.
Do you routinely screen for iron deficiency in non-anemic HFpEF patients?
Or do you still wait for hemoglobin to fall?
Check the infographic (generated with NotebookLM) for a visual synthesis.
Key references:
- Packer M. JACC 2025
- EHJ 2024 (FAIR-HFpEF)
- JAMA 2017 (IRONOUT HF)”
Article 1: The Adipokine Hypothesis of Heart Failure With a Preserved Ejection Fraction: A Novel Framework to Explain Pathogenesis and Guide Treatment
Author: Milton Packer
Read the Full Article on JACC

Article 2: Ferric carboxymaltose and exercise capacity in heart failure with preserved ejection fraction and iron deficiency: the FAIR-HFpEF trial
Authors: Stephan von Haehling , Wolfram Doehner , Ruben Evertz , Tania Garfias-Veitl , Carlotta Derad , Monika Diek , Mahir Karakas , Ralf Birkemeyer , Gerasimos Fillippatos , Mitja Lainscak , Javed Butler , Piotr Ponikowski , Michael Böhm , Tim Friede , Stefan D Anker
Read the Full Article on European Heart Journal

Article 3: Effect of Oral Iron Repletion on Exercise Capacity in Patients With Heart Failure With Reduced Ejection Fraction and Iron Deficiency. The IRONOUT HF Randomized Clinical Trial
Authors: Gregory D. Lewis, Rajeev Malhotra, Adrian F. Hernandez, Steven E. McNulty, Andrew Smith, G. Michael Felker, W. H. Wilson Tang, Shane J. LaRue, Margaret M. Redfield, Marc J. Semigran, Michael M. Givertz, Peter Van Buren, David Whellan, Kevin J. Anstrom, Monica R. Shah, Patrice Desvigne-Nickens, Javed Butler, Eugene Braunwald, for the NHLBI Heart Failure Clinical Research Network
Read the Full Article on JAMA

Stay updated with Hemostasis Today.
{kind=link}
-
Jul 5, 2026, 22:51Shahzaib Akram: What Are We Actually Seeing When a Sickling Test Goes Positive?
-
Jul 5, 2026, 21:474 Tips for Exercising with A Bleeding Disorder – Haemophilia Foundation Australia
-
Jul 5, 2026, 21:06Heghine Khachatryan: Toward Personalized Management of Glanzmann Thrombasthenia
-
Jul 5, 2026, 21:06Priyanka Kumari: IV Fluids and Isotonic Solution
-
Jul 5, 2026, 21:05Ahmed Rizq: Would You Thrombolyse a Stable Patient?
-
Jul 5, 2026, 21:03Emmanuel Obeng Ofori: Diagnosing Anaemia – Why Treating the Root Cause Matters More Than Simply Raising the Haemoglobin
-
Jul 5, 2026, 21:02Mohit Koladia: The Pharmacist’s Role in Stroke Prevention for Atrial Fibrillation
-
Jul 5, 2026, 20:22J. Meireles-Brandao: Exploring the Approach to Thrombophillias
-
Jul 5, 2026, 20:13Kavya Keerthana: The Platelet Count Everyone Calls ‘Reactive’ Until It Isn’t