

Deepak Yadav: What 2025 Evidence Tells Us About Stroke Care
Deepak Yadav, Consultant and Assistant Professor of Neurology at Amrita Hospital, shared on LinkedIn:
”Stroke Care Just Changed: What 2025 Evidence Tells Us (And Why It Matters)
Stroke medicine is moving fast — and 2025 quietly rewrote several ‘assumed truths.’
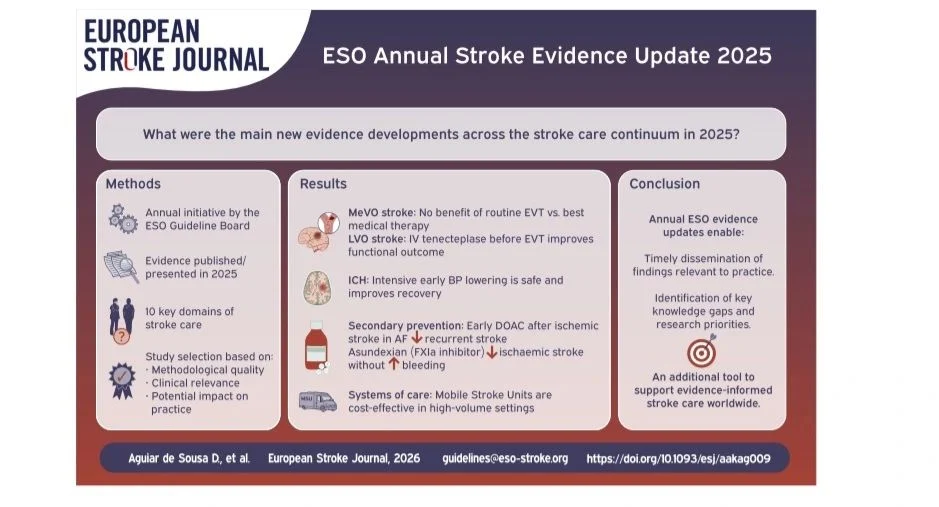
The European Stroke Organisation (ESO) Annual Stroke Evidence Update 2025 synthesised the most practice-changing trials across acute care, prevention, rehab, cognition, and systems of care
Acute Ischemic Stroke: Less Is More
Endovascular thrombectomy (EVT)
NO routine benefit for MeVO strokes
Medical therapy (including IV thrombolysis when eligible) remains the backbone
Bigger is not always better intervention
Tenecteplase (TNK)
TNK before thrombectomy improves 90-day functional outcomes
Higher early recanalisation vs alteplase
TNK is now strongly reinforced as bridging therapy
Late-window thrombolysis (4.5–24 h)
Can help highly selected patients using advanced imaging
Tissue > time, but selection is everything
Intracerebral Haemorrhage (ICH): TIME equals BRAIN
Blood pressure control
Early, intensive BP lowering (<140 mmHg) is SAFE
Best outcomes when started within 3 hours. Delay here = lost recovery
Post-ICH prevention
Low-dose polypill strategy achieved SBP ≈127 mmHg
Reduced recurrent stroke without added harm
Simple combinations beat therapeutic inertia
Secondary Prevention: Old Dogmas Fall
Atrial fibrillation
Early DOAC initiation (≤4 days) ↓ recurrent stroke
Adding antiplatelet therapy? More bleeding, no benefit
ESUS
Anticoagulation still does NOT beat aspirin, Precision is better than empiricism
Factor XIa inhibition (Asundexian)
Infrequent ischaemic stroke without more bleeding
Works in non-cardioembolic stroke / high-risk TIA
A glimpse of safer antithrombotic future
Cognition and Life After Stroke
Post-stroke dementia
Risk continues for YEARS
Metabolic syndrome equals major modifiable driver
Acute reperfusion- lower dementia risk by ~65%
What helps cognition?
- Computerised cognitive training
- Brain stimulation
- Cardiorespiratory exercise
Stroke care does not equal discharge care
Systems of Care: Organisation saves Neurons
- Mobile Stroke Units
Improve outcomes
Cost-effective in high-volume systems
- Workflow optimisation
Behaviour-change packages – lower door-to-puncture time
Better 90-day outcomes
Process design is a treatment
What Everyone Should Know
- EVT – not for all vessel occlusions
- Tenecteplase is gaining ground
- BP control after ICH is urgent, not optional
- Early anticoagulation in AF is safer than we thought
- Stroke recurrence risk remains high for years
- Cognition and rehabilitation are not ‘extras’
- Systems and workflows save as many lives as drugs
Final Thought
Stroke care is no longer about doing more — It’s about doing the right thing, faster, for the right patient.
Source: European Stroke Organisation – Annual Stroke Evidence Update 2025 (European Stroke Journal, 2026)”

Stay updated with Hemostasis Today.
{kind=link}
-
Jul 13, 2026, 10:25Flora Peyvandi: A Practical Approach to ALT Elevation After Gene Therapy at ISTH 2026
-
Jul 13, 2026, 10:02Jessica Garcia: Where Science and Community Come Together at ISTH 2026
-
Jul 13, 2026, 09:46Fabrice Cognasse: Is There Such a Thing as the Perfect Platelet Product?
-
Jul 13, 2026, 09:42Cancer-Associated Arterial Thromboembolism: Redefining the Thrombotic Burden in Oncology
-
Jul 13, 2026, 05:59Connecting and Collaborating at ISTH 2026 – NNHF
-
Jul 13, 2026, 05:58Lara Monica: Back at ISTH – Looking Forward to Science and Reconnections!
-
Jul 13, 2026, 05:57Barbara Adams Krolak: Exciting Updates From the ISTH 2026 Regulatory Session
-
Jul 13, 2026, 05:57Alberto Maino: ISTH 2026 Has Just Begun
-
Jul 13, 2026, 05:56Karin Knobe: Fresh Insights and Familiar Faces from ISTH 2026