

Peter Antevy: Revealing How SWiFT Is Highlighting Prehospital System Limitations
Peter Antevy, Founder and Chief Medical Officer at Handtevy, President of C3MD, EMS Medical Director at Davie Fire Rescue, shared a post on LinkedIn:
“A closer look at the numbers behind the NEJM’s latest whole blood trial
The call comes in. Stabbing, unresponsive. Your crew is on scene in four minutes. Blood is hanging before the patient hits the stretcher. First unit is flowing within eight minutes of EMS contact. You are at the trauma center in under twenty minutes from the 911 call. The patient’s systolic blood pressure on your arrival was 68. By the time you push through the trauma bay doors, it is 94. The patient survives.
Now imagine a different system. The helicopter team arrives at the scene a median of 67 minutes before the patient reaches the emergency department. The median systolic blood pressure on arrival is 95 mmHg. The 30-day mortality, even after excluding patients who arrested in the field, is 27%. And from this system, a major trial is published in The New England Journal of Medicine, concluding that prehospital whole blood offers no benefit over component therapy
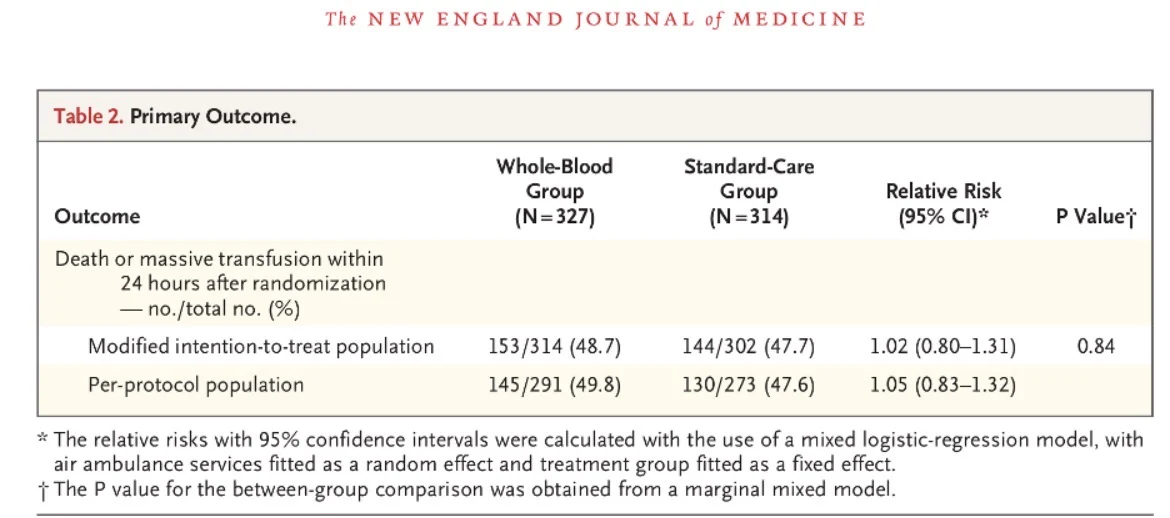
The SWiFT trial (Study of Whole Blood in Frontline Trauma), published March 17, 2026, randomized 942 patients across 10 air ambulance services in England to receive either up to 2 units of whole blood or standard care with red cells and plasma before hospital arrival. The primary outcome was a composite of death or massive transfusion within 24 hours. The result: 48.7% in the whole blood group versus 47.7% in the standard care group. No difference. The authors concluded that prehospital whole blood was not superior to component therapy.
Within hours of publication, the medical press ran headlines declaring whole blood no better than components. Those headlines will reach every EMS medical director in the country. The data beneath them tell a very different story.
This is a well-conducted trial from a rigorous group of investigators. But the question it answers is narrow, and the system in which it was conducted is not generalizable to most American EMS systems. The data within the paper itself reveal why.
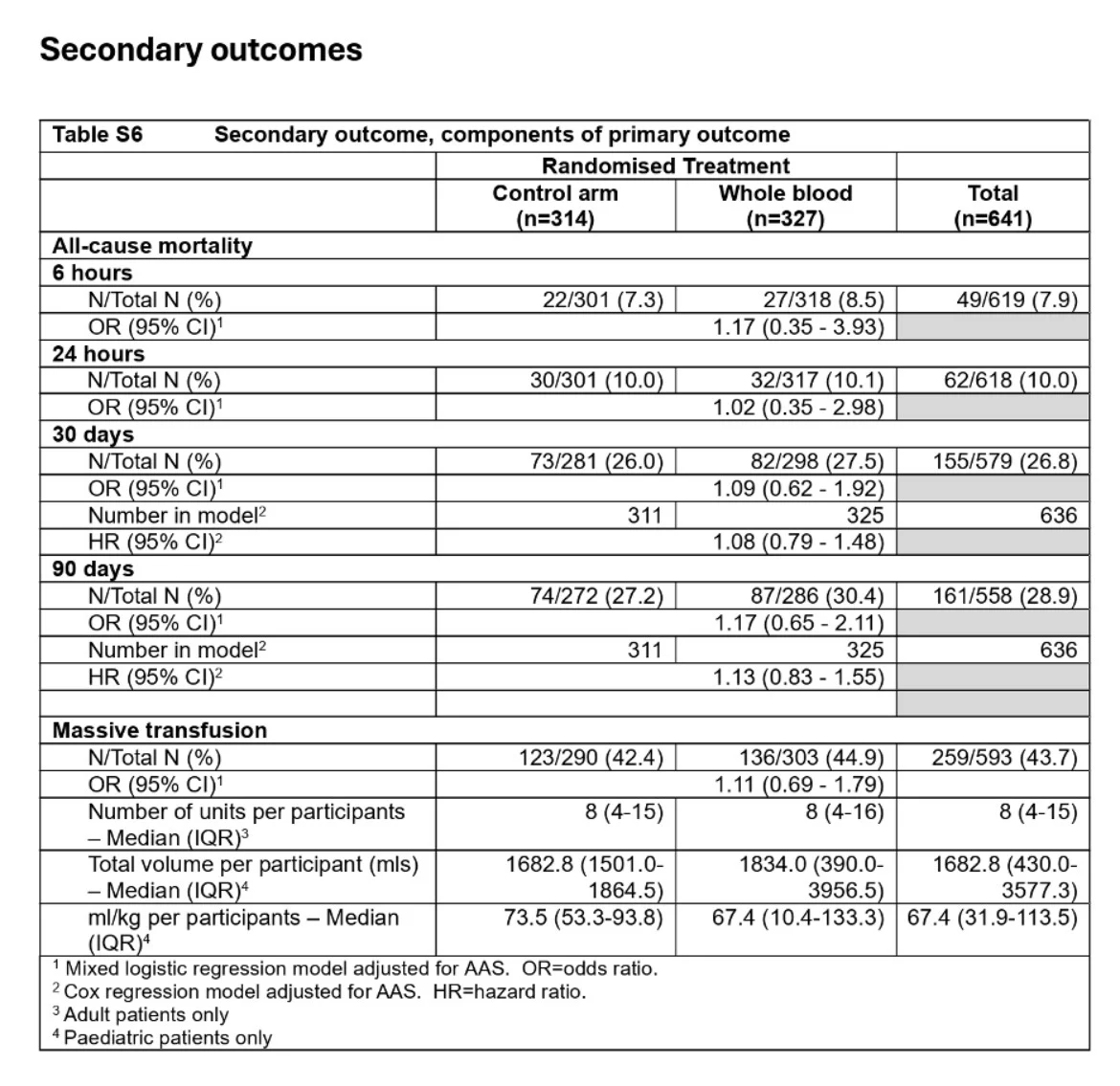
Start with the primary outcome. The investigators chose a composite endpoint: death from any cause OR massive transfusion (defined as 10 or more units of blood products) within 24 hours. When you look at the actual mortality numbers, only about 10% of patients in each group died within 24 hours (32 of 317 in the whole blood group, 30 of 301 in the standard care group). The composite event rate of nearly 48% was driven overwhelmingly by massive transfusion, not death. The headline number is inflated by a surrogate outcome that may not reflect what clinicians and patients care most about.
Massive transfusion itself, defined as receiving 10 or more units in 24 hours, introduces a well-known survival bias. You have to live long enough to receive 10 units. A patient who exsanguinates in the field or dies within minutes of hospital arrival never reaches that threshold. The definition systematically excludes the sickest patients from the outcome it is supposed to measure.
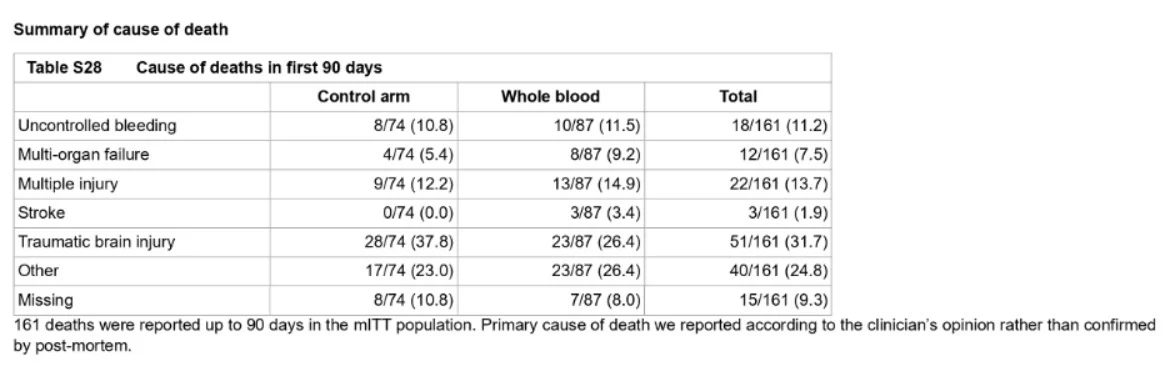
Now look at the cause of death data, buried in the supplementary appendix. Of the 161 patients who died within 90 days across both groups, only 18 (11.2%) died from uncontrolled bleeding. Traumatic brain injury accounted for 31.7% of deaths. ‘Multiple injury’ and ‘other’ causes accounted for another 38.5%. If fewer than 12% of deaths are from hemorrhage, you are studying a population in which the dominant cause of death cannot be modified by any transfusion strategy, whole blood or otherwise.
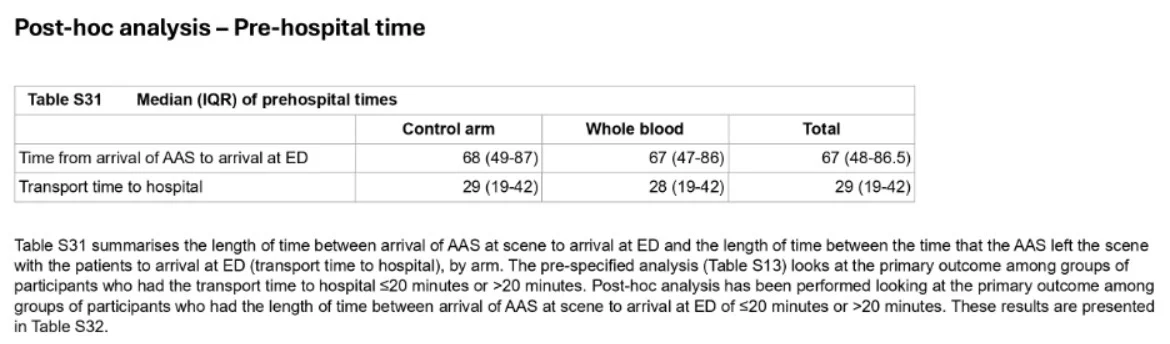
The prehospital time intervals tell a striking story. The supplementary data report the median time from arrival of the air ambulance service at the scene to arrival at the emergency department: 67 minutes (IQR 47 to 86.5). The median transport time alone, once the helicopter actually left the scene, was 29 minutes. That means roughly 38 minutes elapsed on scene before departure. And this does not include the time from injury or 911 call to arrival of the air ambulance team, which in the UK system involves a ground ambulance arriving first, followed by the helicopter team as a secondary response.
In the RePhill trial’s authors’ reply letter, they reported a median of 83 minutes from emergency call to ED arrival in that system, with the prehospital critical care team arriving a median of 26 minutes after the initial call. SWiFT does not report the full interval from injury or emergency call to hospital arrival, but based on the architecture of the same system, total prehospital time likely exceeds 90 minutes for many patients.
Compare that to what is happening on the ground in American cities. In Palm Beach County, where Kenneth Scheppke, and I serve as medical directors for Palm Beach County Fire Rescue, we have transfused over 300 units of whole blood through a ground EMS program we built from the ground up and published in 2023 (Charles Coyle et al., Prehospital and Disaster Medicine).
Among 170 patients transfused through early 2025, 70% of penetrating trauma cases were gunshot wounds. Seventy-five percent of cardiac arrest patients had no pulse at the time blood was given. Among patients who had a pulse before transfusion, 84% survived. Our clinicians give calcium in 95% of cases, perform finger thoracostomy in 91%, and administer TXA in 62%. This is a single-agency ground transport system. No helicopters. No 67-minute prehospital intervals. We get blood into patients and get them to the trauma center.
The pattern holds across US programs. In New Orleans, published data from Juan Duchesne and colleagues showed that EMS delivered the first unit of blood a median of 8 minutes after patient contact in penetrating trauma patients with systolic blood pressure at or below 90 mmHg. Those patients had a 7% in-hospital mortality rate, compared to 29% in a historical cohort that received blood only after hospital arrival.
In Atlanta, Grady Health System reported 83% survival at 24 hours and 80.8% at 30 days in a cohort of 375 patients receiving prehospital whole blood via ground transport. In Washington, DC, the fire department’s whole blood program reported a 92% survival rate for transfused patients not in cardiac arrest. These are systems where the philosophy is simple: get blood into the patient immediately, control the bleeding, and move.
The patient populations are also fundamentally different. In SWiFT, the median prehospital systolic blood pressure was 95 mmHg. Nearly half the patients had a Glasgow Coma Scale score of 13 or greater. The median Injury Severity Score was 33, which represents profoundly injured patients, but the hemodynamic profile suggests many were not in frank hemorrhagic shock at the time of the prehospital intervention.
In the New Orleans data, patients had penetrating injuries with systolic pressures at or below 90. In the DC program, the majority of transfusions were for penetrating trauma. These are patients who are actively exsanguinating in the field, not patients with a systolic of 95 and a GCS of 12.
And yet the SWiFT population, despite appearing hemodynamically more stable, had a 27% 30-day mortality rate (excluding prehospital cardiac arrests). That is a strikingly poor outcome for a cohort with a median systolic of 95. It raises a serious question about the system itself: are prolonged prehospital times contributing to worse outcomes regardless of what type of blood product is being transfused?
The trial was also designed as whole blood versus components, not blood versus no blood. Both arms received prehospital transfusion. The dose was limited to 2 units, a constraint acknowledged by the authors as potentially insufficient to detect a treatment effect. The whole blood units were stored up to 21 days, meaning the plasma within them had degraded coagulation factors compared to the thawed or lyophilized plasma in the control arm, which was typically less than 5 days old. This likely explains the paradoxical finding that prothrombin times were more frequently elevated in the whole blood group (40.7% versus 30.5%).
The authors themselves note this finding had no clinical significance, but it does suggest the comparison was not between fresh whole blood and components. It was between old whole blood and relatively fresh components. As I discussed in a recent post on the THOR Network transfusion guidelines, the quality and timing of blood product delivery matter enormously.
There is one finding the trial does support clearly. Whole blood had fewer serious adverse events than component therapy (31 versus 37 events). No transfusion-associated adverse events occurred in the whole blood group. The safety profile favors whole blood, or at minimum shows equivalence, which reinforces its logistical advantages: a single bag, simpler storage, faster administration, and reduced risk of transfusion error in a chaotic prehospital environment.
This trial joins RePhill in a pattern of UK helicopter-based prehospital transfusion studies that show no benefit. RePhill compared red cells and lyophilized plasma to normal saline and also found no difference, in a system where the median time from emergency call to emergency department arrival was 83 minutes. At some point, we have to ask whether the problem is the intervention or the system testing it.
The SWiFT trial tells us that in a system with prolonged prehospital times, limited transfusion doses, and a patient population in which fewer than 12% of deaths are from hemorrhage, switching from component therapy to 2 units of stored whole blood does not change outcomes. It does not tell us whether prehospital whole blood saves lives in fast urban ground EMS systems where blood reaches exsanguinating patients within minutes of injury. That is a fundamentally different question, and the answer is being written every day in the streets of New Orleans, Atlanta, Washington, San Antonio, Palm Beach County, and dozens of other American cities.
The next generation of evidence will not come from 90-minute helicopter transports. It will come from the systems getting blood to patients the fastest.”
Title: Prehospital Whole Blood in Traumatic Hemorrhage — a Randomized Controlled Trial
Authors: Jason E. Smith, Rebecca Cardigan, Emily Sanderson, Laura Silsby, Claire Rourke, Ed B.G. Barnard, Peter Basham, Grazia Antonacci, Richard Charlewood, Nikki Dallas, Jane Davies, Elizabeth Goodwin, Annie Hawton, Cara Hudson, Joanne Lucas, Katie Keen, Richard M. Lyon, Brodie Nolan, Gavin D. Perkins, Viona Rundell, Laura Smith, Simon J. Stanworth, Anne Weaver, Tom Woolley, Laura Green
Read the Full Article on The New England Journal of Medicine

Stay updated on all scientific advances with Hemostasis Today.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-
Aug 11, 2026, 05:53Isaac Okello: Strengthening Sickle Cell Advocacy in Uganda
-
Aug 11, 2026, 05:38Rami Unterman: A Simple New Biomarker for Fibrotic ILDs
-
Aug 11, 2026, 04:10Haroun Gajraj: CLaCS vs Sclerotherapy – What Does the Evidence Show
-
Aug 11, 2026, 02:54Tareq Abadl: The Ultimate Guide to Clinically Significant Antibodies
-
Aug 10, 2026, 17:35Chokri Ben Lamine: Balancing Holistic Care and Precision in Hematology
-
Aug 10, 2026, 17:14Anna Stanizzi: Patient Blood Management as a New Model of Personalized Care
-
Aug 10, 2026, 17:12Odong Christopher: New Research on Ischemic Stroke Prediction in Uganda
-
Aug 10, 2026, 16:58Jeff Szer AM: Advancing the Management of Paroxysmal Nocturnal Hemoglobinuria
-
Aug 10, 2026, 16:51Suebsarn Ruksakulpiwat։ A New Milestone in the Development of the Stroke Risk Screening Scales