

Ney Carter Borges: Clinical Cardiovascular Polygenic Risk Report for 8 Conditions
Ney Carter Borges, Member Cardiologist of Global Physician Association at Cleveland Clinic Florida, shared a post on LinkedIn about a recent article by Anika Misra et al. published in JACC Journals, adding:
“Clinical Cardiovascular Polygenic Risk Report for 8 Conditions
Bottom line: strong methodological paper, clinically relevant, but still first-generation. Best used as an adjunct to traditional risk assessment, not as a standalone decision tool.
This JACC article evaluates whether polygenic risk scores can move from research into real clinical practice.
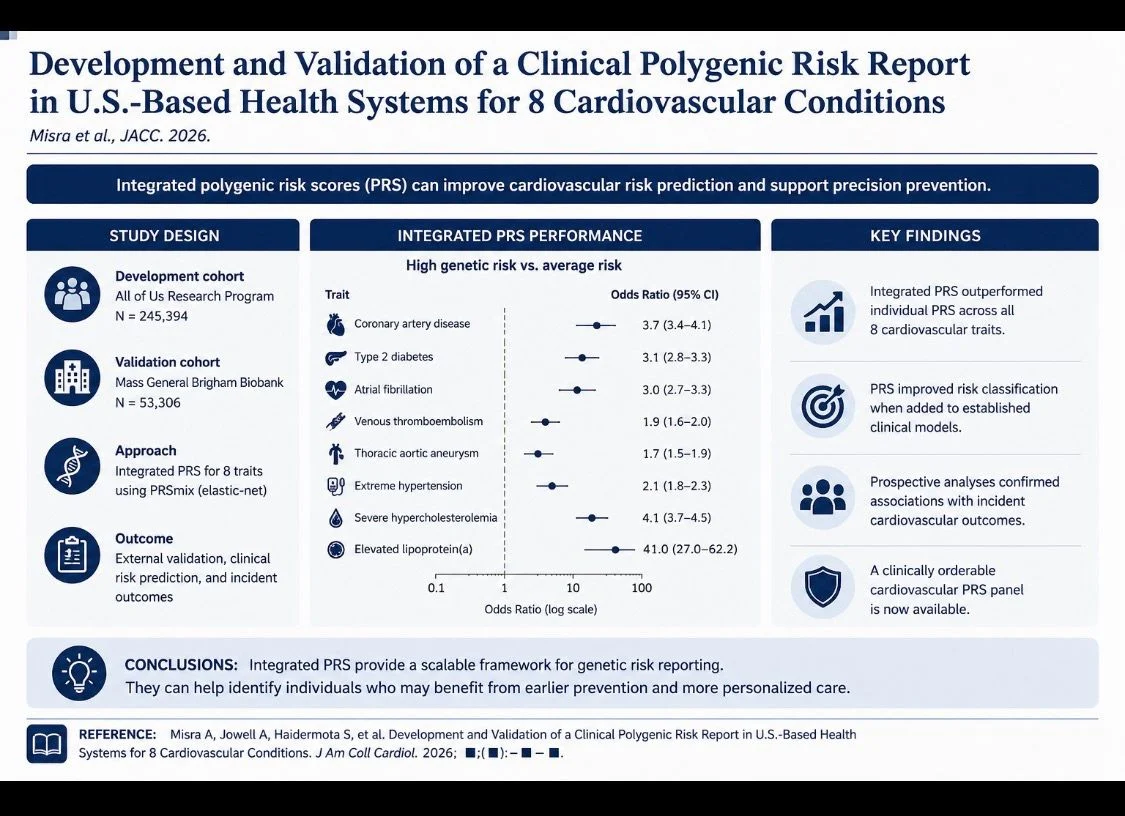
The authors developed and validated an integrated cardiovascular PRS panel for eight conditions: coronary artery disease, atrial fibrillation, type 2 diabetes, venous thromboembolism, thoracic aortic aneurysm, severe hypercholesterolemia, extreme hypertension, and elevated lipoprotein(a).
The work used very large genomic/EHR datasets:
All of Us for development, Mass General Brigham Biobank for external validation, and UK Biobank for Lp(a) modeling.
The central strength is clinical translation. Instead of testing isolated PRS models, the authors created an integrated, reportable, clinician-orderable cardiovascular genetic risk panel.
This is important because a single genotyping assay can generate multiple risk estimates, potentially identifying inherited cardiovascular vulnerability before traditional risk factors become abnormal.
Statistically, the strongest results were seen for Lp(a), severe hypercholesterolemia, CAD, type 2 diabetes, and atrial fibrillation.
In Mass General Brigham, high genetic risk versus average risk showed ORs of 3.7 for CAD, 3.1 for T2DM, 3.0 for AF, 4.1 for severe hypercholesterolemia, and an exceptionally high OR of 41.0 for elevated Lp(a).
More modest associations were seen for VTE, TAA, and extreme hypertension.
Clinically, the most practical message is not that PRS replaces standard risk calculators, but that it may improve risk classification.
The study showed net reclassification improvement when PRS was added to CHARGE-AF, PCE, and PREVENT models.
This suggests that some patients labelled ‘borderline’ or ‘intermediate’ by traditional tools may actually carry genetically high lifetime risk.
The article is also honest about limitations. PRS performance remains weaker in non-European ancestry groups, reflecting the broader problem that most PRS were developed mainly in European populations.
Calibration also differed between population-based cohorts and health-system cohorts, meaning absolute risk estimates may not transfer perfectly between settings.”
Title: Development and Validation of a Clinical Polygenic Risk Report in U.S.-Based Health Systems for 8 Cardiovascular Conditions
Authors: Anika Misra, Amanda Jowell, Sara Haidermota, Emma Perez, Lisa Mahanta, Kimberly J. O’Brien, Anna Nagy, Limin Hao, Buu Truong, Krishna Aragam, Akl C. Fahed, Shaan Khurshid, Patrick T. Ellinor, Anna C.F. Lewis, Niall Lennon, Whitney Hornsby, Matthew S. Lebo, Elizabeth W. Karlson, Pradeep Natarajan, Aniruddh P. Patel

Other posts featuring Ney Carter Borges on Hemostasis Today.
{kind=link}
-
Jun 27, 2026, 14:01Abdul Mannan: DOACs in Cancer-Associated VTE – When to Avoid Them, And When LMWH Wins
-
Jun 27, 2026, 14:01Francesca Palandri: Highlighting Innovation in Rare Disease Care at EHA 2026
-
Jun 27, 2026, 13:51Mubariz Ahsan: Trends in Stroke Mortality in Peripheral Artery Disease from CDC WONDER Study
-
Jun 27, 2026, 13:40Naveen Pemmaraju: Pacritinib Versus Momelotinib in Thrombocytopenic Myelofibrosis
-
Jun 27, 2026, 13:27Limited-Time Open Access for the EAHAD 2026 Joint Session with ISTH – EAHAD
-
Jun 27, 2026, 13:16Stefano Rivella: Stress Erythropoiesis and the Role of HRG1-Mediated Heme Import
-
Jun 27, 2026, 13:10Yahya Samadi: Luspatercept Shows Promise in Reducing Transfusion Burden in β-Thalassemia
-
Jun 27, 2026, 13:03Margarida Marreiros: Supporting Excellence in Hemostasis Testing
-
Jun 27, 2026, 12:44Maia Meier: Turning Achievement into Advocacy for Women with Bleeding Disorders