

Alen Emmanuel Joshy/LinkedIn
Dec 20, 2025, 23:44
Alen Emmanuel Joshy: CT Brain in Intracranial Hemorrhage
Alen Emmanuel Joshy, MRI Technician at AKG Memorial Cooperative Hospital, shared on LinkedIn:
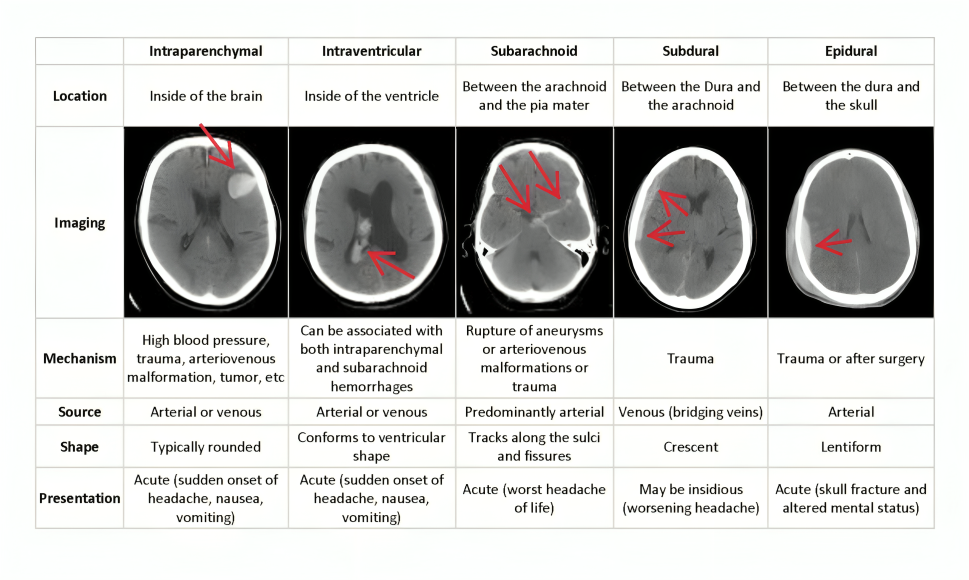
”CT Brain in Intracranial Hemorrhage
Technical and Protocol Points:
- Non-contrast CT (NCCT) is mandatory initially — contrast can obscure acute blood.
- Thin slices (≤5 mm, preferably 1–2 mm) improve detection of small bleeds.
- Bone window helps identify associated skull fractures.
- Repeat CT is crucial in deteriorating patients to assess bleed progression.
Density and Physics Insight:
- Acute blood appears hyperdense (60–80 HU) due to high protein and iron content.
- Density reduces over time due to clot lysis and dilution by CSF.
- Hematocrit level influences bleed conspicuity on CT.
Evolution of Hemorrhage on CT:
- Hyperacute (<6 hrs): May appear heterogeneous due to active bleeding (“swirl sign”)
- Acute (6 hrs–3 days): Homogeneously hyperdense
- Early chronic: Peripheral membrane formation may be seen
Signs Suggesting Active or Severe Bleed:
- Swirl sign: Hypodense area within hyperdense clot → ongoing bleeding
- Spot sign (on CTA): Predictor of hematoma expansion
- Mass effect disproportionate to bleed size
Important Secondary Effects:
- Raised intracranial pressure (ICP)
- Herniation (subfalcine, transtentorial, tonsillar)
- Acute obstructive hydrocephalus (especially with IVH or SAH)
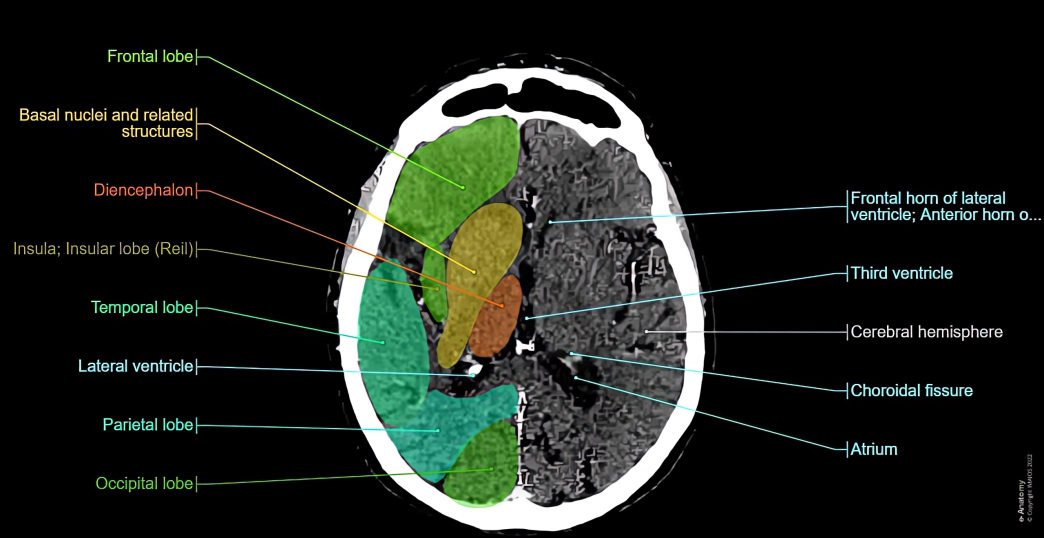
Etiology Clues Based on Location:
- Basal ganglia bleed: Hypertension
- Lobar hemorrhage: Amyloid angiopathy, tumor, anticoagulation
- Cerebellar bleed: Life-threatening due to brainstem compression
- Temporal lobe bleed: Consider trauma or aneurysmal SAH extension
When to Add CT Angiography?
- Suspected aneurysm or AVM
- Young patient with no hypertension
- Lobar hemorrhage without trauma
- SAH with negative NCCT after 6 hours
Pitfalls and Mimics on CT:
- Calcifications vs acute bleed
- Beam-hardening artifacts
- Contrast staining post-procedure
- Dense venous sinuses mimicking SAH
Clinical Correlation Matters:
- Sudden severe headache → rule out SAH
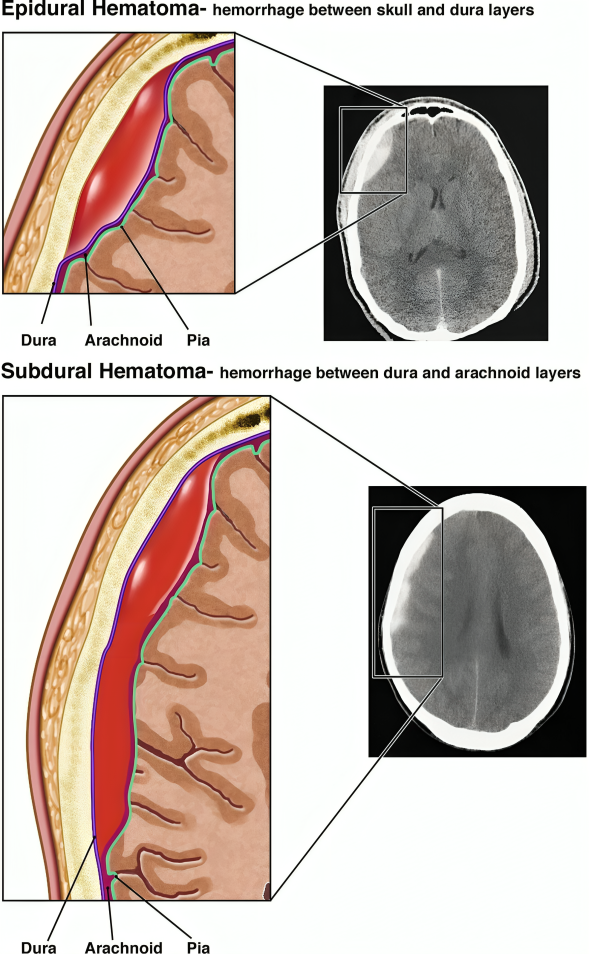
- Trauma with lucid interval → EDH
- Elderly with minor trauma → SDH
- Anticoagulated patients → high risk of expansion
Take-Home Message:
- CT brain not only detects hemorrhage but also predicts severity, guides management, and helps identify the cause. Early recognition saves lives.”

Stay informed with Hemostasis Today.
{kind=link}
{kind=link}
{kind=link}
-
Jul 9, 2026, 14:49Celebrating a Century of von Willebrand Disease Research and Care – Seminars in Thrombosis and Hemostasis
-
Jul 9, 2026, 14:38Valance Washington: International Hemostasis Community Prepares for GRC 2026
-
Jul 9, 2026, 14:27Dima Shulkin: Next-Generation AI Models Improve Early Sepsis Recognition
-
Jul 9, 2026, 14:12Omar Hajji: Seasonal Determinants of Mortality in Sepsis and Cardiogenic Shock
-
Jul 9, 2026, 13:54Hussein Yassine: Why Omega-3s May Fall Short in Preventing Alzheimer’s Disease
-
Jul 9, 2026, 13:16Olivier Mathieu: Innovating the Future of Hemostasis at ISTH 2026
-
Jul 9, 2026, 12:41Thomas Palmer-Dench: Hexokinase Controls Platelet Activation and Hemostasis
-
Jul 9, 2026, 12:19Paschalis Evangelidis: Join Our Special Issue on Thrombosis and Vascular Disorders
-
Jul 9, 2026, 12:16Fernanda Betti Solano: Could Iron Deficiency Be Affecting Your Sleep?