

Nasr Almusattar: What is the No-Reflow Phenomenon?
Nasr Almusattar, Anesthesiologist Assistant, shared a post on LinkedIn:
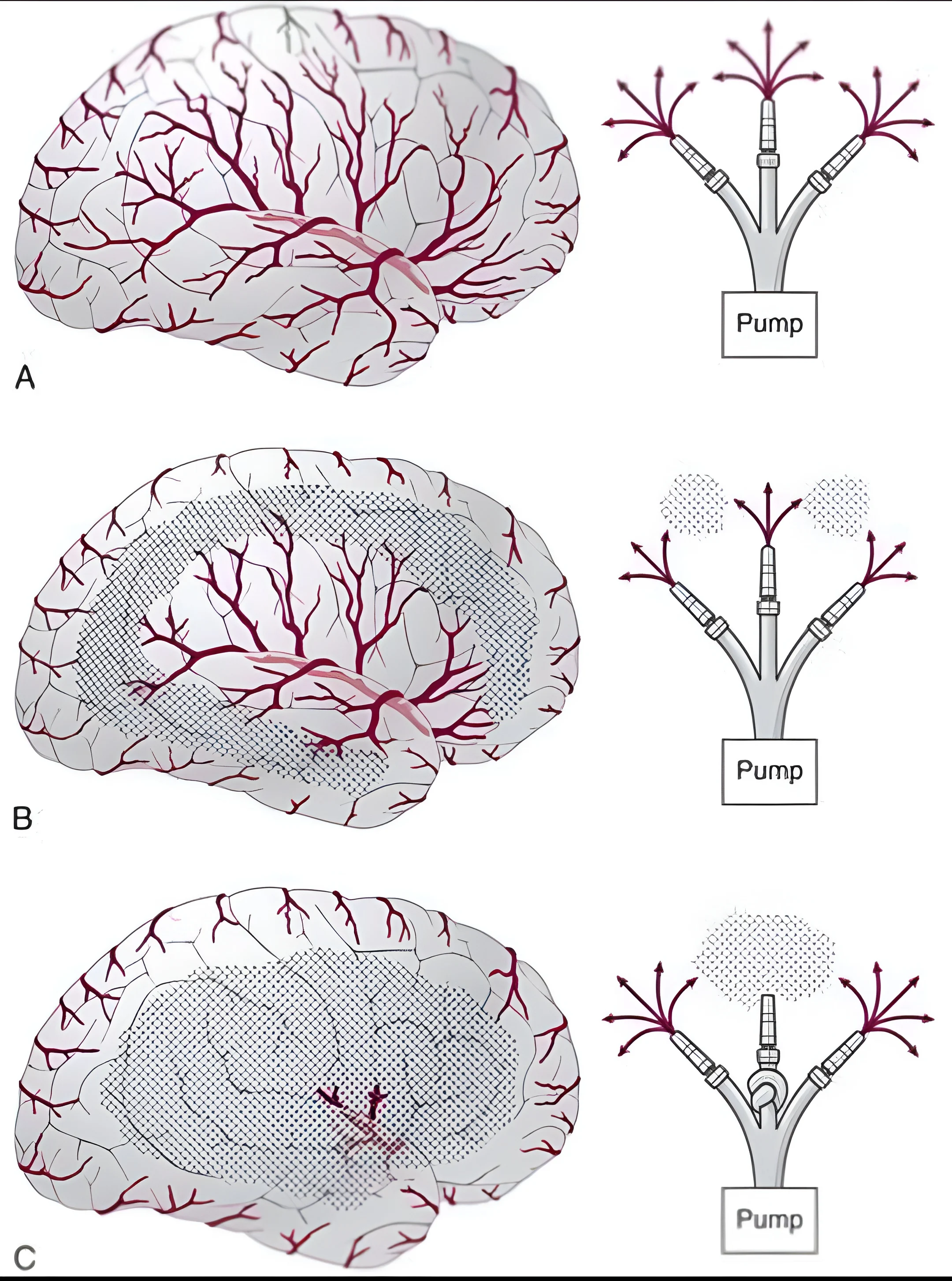
“What is the No-Reflow Phenomenon?
The no-reflow phenomenon refers to the failure of microvascular perfusion despite successful restoration of blood flow in the major vessels.
In other words:
The artery is open, but blood does not reach the tissues at the capillary level.
It is a critical issue observed after Cardiopulmonary Bypass (CPB), affecting both the heart and the brain.
Pathophysiology (Why does it happen?)
- No-reflow is mainly caused by microcirculatory dysfunction, due to:
- Ischemia – Reperfusion Injury – Production of reactive oxygen species (ROS)
- Endothelial Dysfunction – Reduced nitric oxide – vasoconstriction
- Capillary Obstruction – Platelets, leukocytes, and microemboli block small vessels
- Cellular Edema – Swelling compresses capillaries
- Increased Blood Viscosity – Impairs microcirculatory flow
Cardiac No-Reflow
- Occurs after restoring coronary circulation.
- Clinical effects:
- Poor myocardial contractility
- Arrhythmias
- Low cardiac output
- Elevated lactate
Cerebral No-Reflow:
- Occurs after restoration of cerebral perfusion.
- Clinical effects:
- Delayed awakening
- Confusion or delirium
- Neurological deficits
Diagnosis:
There is no single test, but clues include:
- Lactate levels
- Persistent organ dysfunction despite adequate flow
- Echocardiography (cardiac dysfunction)
- Cerebral oximetry (NIRS) if available
Management:
- Management is supportive and multi-targeted
1. Optimize Hemodynamics
Maintain adequate MAP (65–80 mmHg)
Ensure sufficient cardiac output
2. Improve Microcirculation
Vasodilators (e.g., Nitroglycerin)
Reduce vasoconstriction
3. Reduce Blood Viscosity
Maintain optimal hematocrit (≈22–28%)
4. Prevent Microthrombosis
Adequate anticoagulation (Heparin during CPB)
5. Control Metabolic Factors
Normalize oxygenation, CO₂, glucose, and electrolytes
6. Organ Support
- Heart: Inotropes (e.g., Dobutamine)
- Brain: Maintain cerebral perfusion pressure
Prevention (Most Important)
During CPB:
- Minimize cross-clamp and bypass time
- Use proper cardioplegia
- Ensure effective de-airing (avoid microemboli)
- Use filters in the circuit
Physiological Control:
- Maintain adequate blood pressure and flow
- Avoid extreme hemodilution
- Control temperature (mild hypothermia)
- Monitor electrolytes and glucose.”

Stay updated with Hemostasis Today.
{kind=link}
-
Aug 11, 2026, 13:47Why Stroke Risk Changes During Pregnancy – International Journal of Stroke
-
Aug 11, 2026, 13:43Moyahabo Julius Rampya: Shaping the Future of Stroke Care in Africa
-
Aug 11, 2026, 13:34Brett Hoover: Plaque Burden May Be Key to Predicting MACE Risk
-
Aug 11, 2026, 11:47Rucha Patil: Strengthening Evidence-Based Haemophilia Care Across India
-
Aug 11, 2026, 11:38Maria Hadjidemetriou: The Patient Perspective in Thalassemia Care
-
Aug 11, 2026, 11:04Wolfgang Miesbach: The Critical Need for Tailored Dosing in VWD
-
Aug 11, 2026, 08:20Hasan Abbas Zaheer: Strengthening Universal Access to Safe Blood in Pakistan
-
Aug 11, 2026, 08:07Nicola Pozzi: Advancing Hemostasis Through Scientific Collaboration at Hemostasis GRC
-
Aug 11, 2026, 07:50When Access to Care Changes Everything – WFH