
Chokri Ben Lamine: CVC-Associated UE-DVT and Catheter Removal
Chokri Ben Lamine, Assistant Consultant at King Faisal Specialist Hospital and Research Center, shared a post on X:
”50 pearls | CVC-associated UE-DVT and catheter removal
Credits for sharing: Dr Ruaa Alyamani – KFSHRC
Study:
1. UE-DVT is a common CVC complication in hematologic malignancy
2. Incidence with PICC around 6–7 percent in cancer patients
3. Standard care is anticoagulation if feasible
4. Major dilemma is when to remove the CVC
5. Concern: catheter removal may lead to embolization and PE
6. Evidence before this study was weak and based mainly on expert opinion
7. ISTH suggests 3–5 days of anticoagulation before removal, but evidence level is low
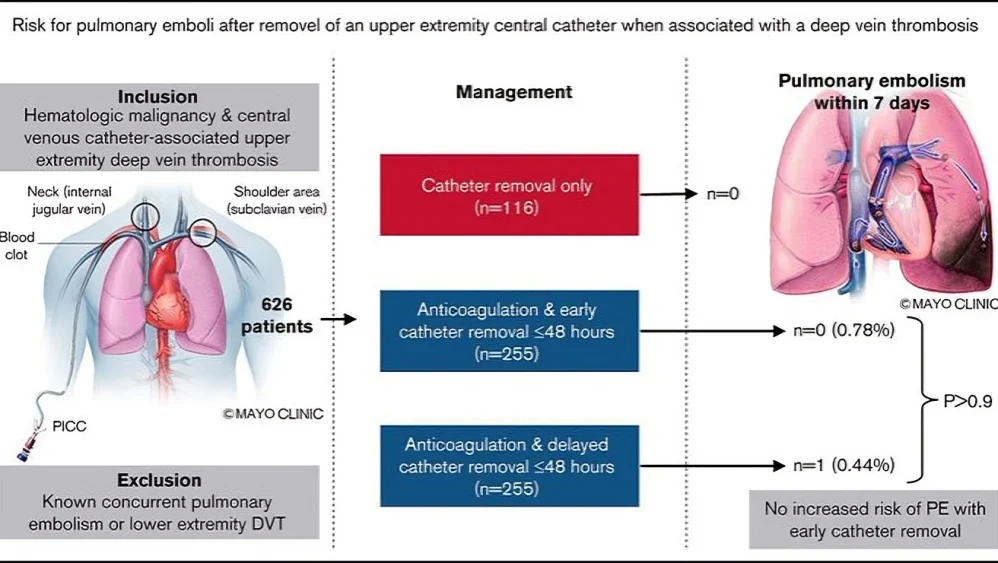
8. Large multicenter cohort including 626 patients with hematologic malignancy
9. 480 patients received anticoagulation
10. 255 underwent early removal within 48 hours
11. 225 had delayed or no removal
12. PE within 7 days:
- Early removal — 0.78 percent
- Delayed or no removal — 0.44 percent
- No statistical difference observed
13. PE or death within 7 days:
- Early removal – 1.18 percent
- Delayed or no removal – 1.33 percent
- Outcomes were equivalent
14. Key clinical takeaway:
Early removal within 48 hours appears safe under anticoagulation
15. No signal that early removal increased PE risk
16. No justification to delay removal solely because of PE concern
17.Findings support practical bedside decision-making
18. Removal-only group without anticoagulation:
19. Zero PE events observed, However, deaths occurred in 2.6 percent
This is not considered a safe overall strategy
20. Important nuance:
- The study evaluated only short-term outcomes over 7 days
- Long-term recurrence was not assessed
21. Prior data suggest removal-only strategies increase recurrence and mortality, Anticoagulation remains the standard approach
22. Thrombocytopenia is a major limitation to anticoagulation in hematology patients
23. This often leads to real-world deviations such as removal only
24. Bleeding and thrombosis risks must be individualized
25. PICCs were the most common catheters associated with UE-DVT
26. Ports were less frequently associated
27. Leukemia and MDS patients carried a higher burden
28. Typical thrombus locations include:
- Subclavian vein
- Internal jugular vein
- Axillary vein
29. PE events mainly originated from proximal veins such as the brachiocephalic vein and SVC
28. Distal UE-DVT carries a lower PE risk
29. Historically, UE-DVT coexists with PE in approximately 9–36 percent of cases
30. Patients with PE at baseline were excluded from this study
31. Anticoagulation options included:
- LMWH, most commonly used in the study
- UFH in ICU or CRRT settings
- DOACs, increasingly used in practice
32. Benefits of anticoagulation extend beyond PE prevention:
- Reduced recurrence
- Reduced post-thrombotic syndrome
33. Risk of post-thrombotic syndrome after UE-DVT is approximately 15–25 percent
34. Chronic morbidity may occur if undertreated
35. Indications for urgent CVC removal include:
- Infection
- Dysfunction
- Catheter no longer needed
36. If the catheter is still required, it can remain in place with anticoagulation
37. Removal is not mandatory in all cases
38. Common clinical myth:
- ‘Early catheter removal causes PE’
- Current data do not support this assumption
39. Actual risk drivers include:
- Clot burden
- Proximal thrombus location
- Underlying hypercoagulability
40.Catheter manipulation alone is not the main driver
41. No routine imaging was performed for asymptomatic PE
- Possible underestimation or overestimation should be considered
42. Some PE events may have existed before catheter removal
- Important for interpretation of results
43. Platelet counts were lower in the no-anticoagulation group
- This reflects real-world practice patterns
44. Bedside decision framework:
- Can the patient tolerate anticoagulation?
- Is the catheter still needed?
- Is there infection present?
45. If anticoagulation is possible, early removal can be performed when needed
46. If anticoagulation is not possible, risk increases
47. Removal-only strategies should be avoided when feasible
48. Optimal management requires multidisciplinary collaboration:
- Hematology
- Vascular medicine
- Infectious disease when line infection is suspected
49. Bottom line:
Do not delay CVC removal solely because of fear of PE if the patient is appropriately anticoagulated.”
Other posts featuring Chokri Ben Lamine on Hemostasis Today.
-
Jun 26, 2026, 18:28Daniel Pereira Monteiro: Why Is Beta Thalassaemia Major so Severe?
-
Jun 26, 2026, 18:27Pradip Pawar: Cell and Gene Therapy – Transforming Medicine in the 21st Century
-
Jun 26, 2026, 18:26Aviva Schwartz: How Can We Better Protect Patients After an Ischemic Stroke?
-
Jun 26, 2026, 18:25Does Reversing Factor Xa Inhibitors Really Carry as Much Thrombotic Risk as We Think? – RPTH Journal
-
Jun 26, 2026, 18:25Akshat Jain: Novel Therapies in Childhood Blood and Cancer Disorders
-
Jun 26, 2026, 16:57Abdul Muqtadir Abbasi: Anticoagulation in DVT Patients With Hidden Varices Requires Extreme Caution
-
Jun 26, 2026, 16:42Anesa Mulabecirovic: Why Von Willebrand Disease Takes Years to Diagnose in Women
-
Jun 26, 2026, 16:32Kaitlin Lichty: A New Identity Reflecting a Shared Legacy of Bleeding Disorders
-
Jun 26, 2026, 16:07Toong Youttananukorn: The WFH Registry Driving Better Care and Advocacy