
Giovanni Solimeno: When the Common Femoral Artery Wall is Diseased, Closure is Not a Step
Giovanni Solimeno, Vascular and Endovascular Surgeon at Pineta Grande Hospital, shared a post on LinkedIn:
“When the Common Femoral Artery wall is diseased, closure is not a step — it’s a part of the endovascular access strategy.
We all love fast hemostasis.
But there’s one scenario where a ‘standard’ closure can become a trap:
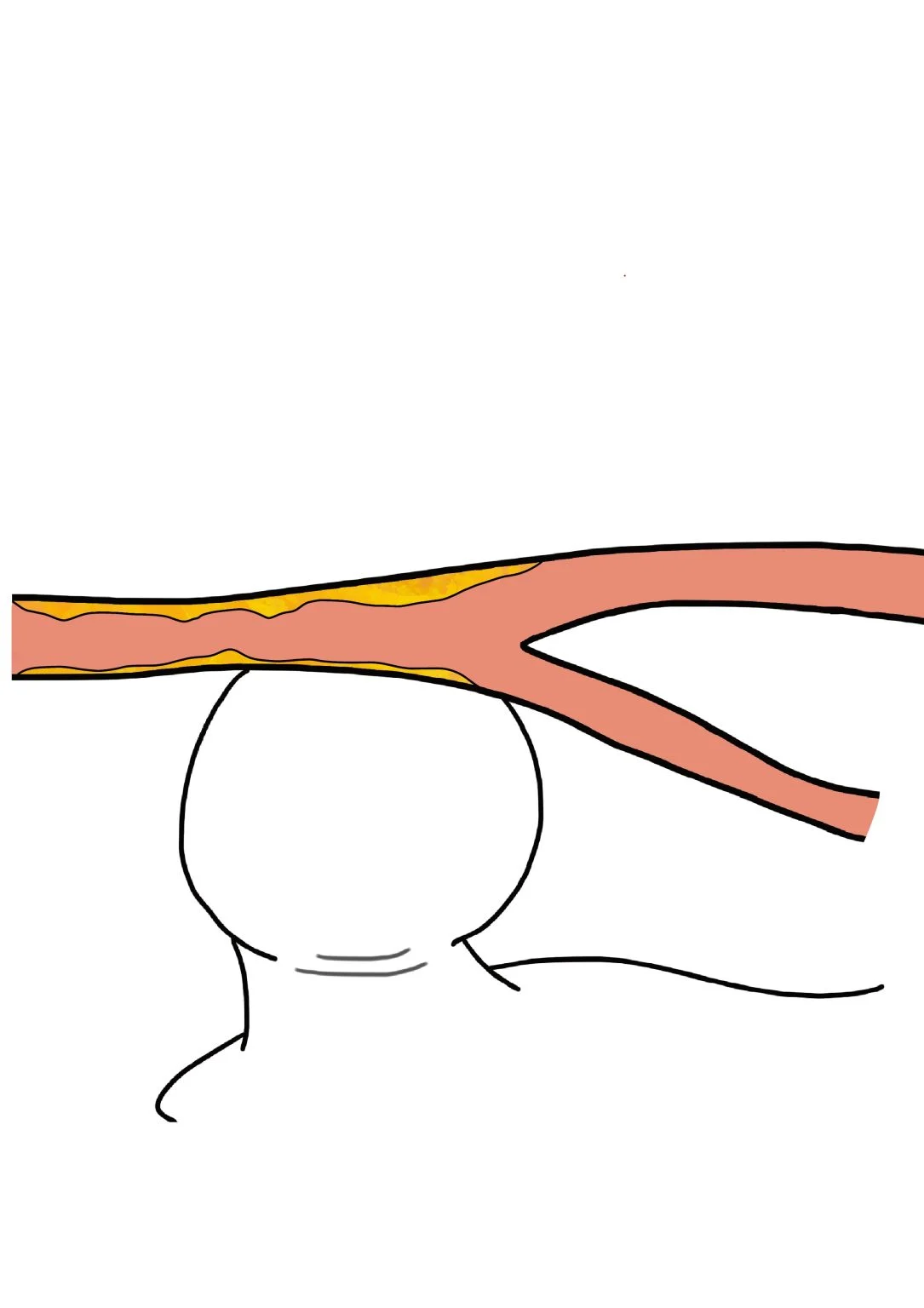
a patent, non-critical CFA… with a truly diseased wall.
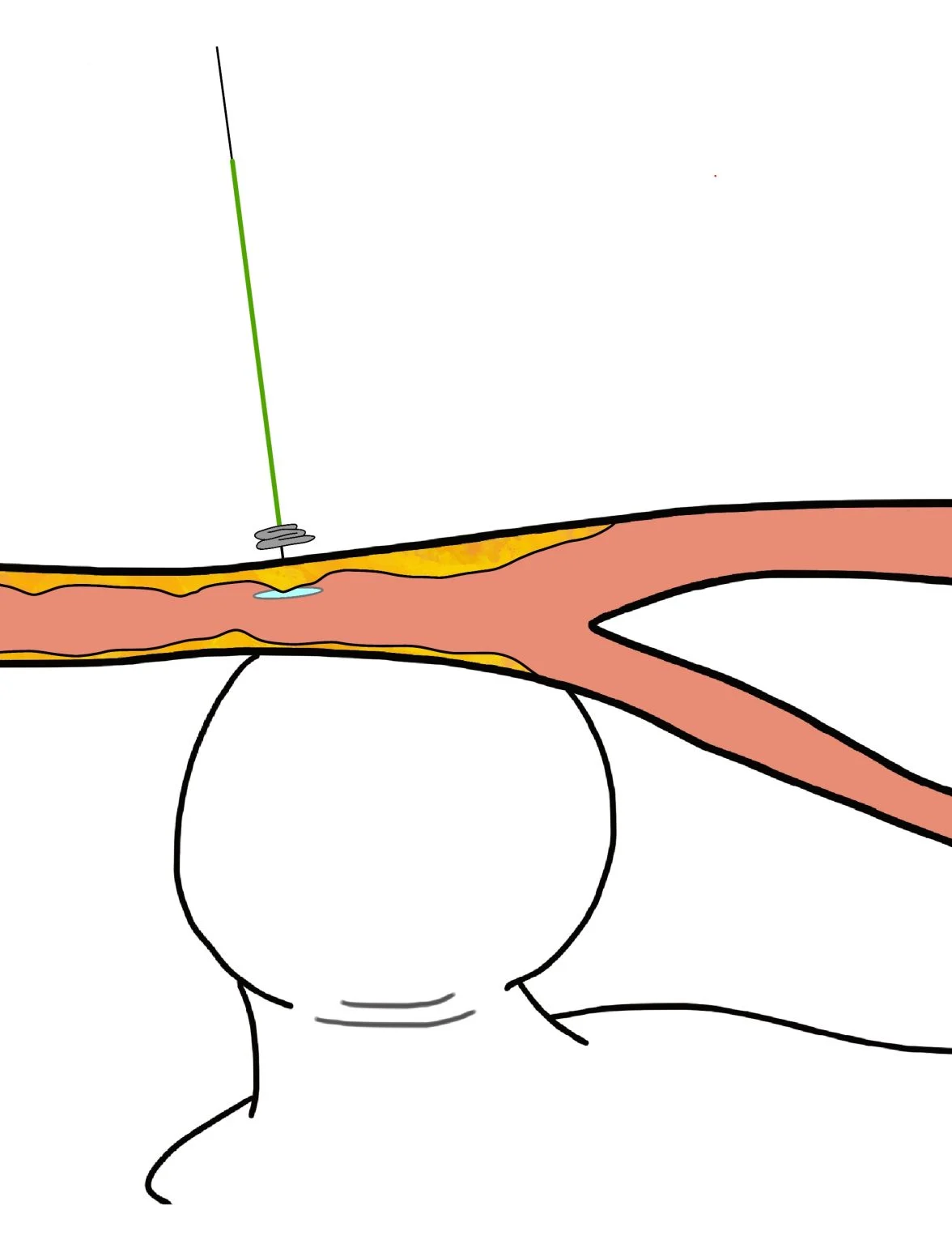
Here’s the mechanism (simple, but easy to underestimate):
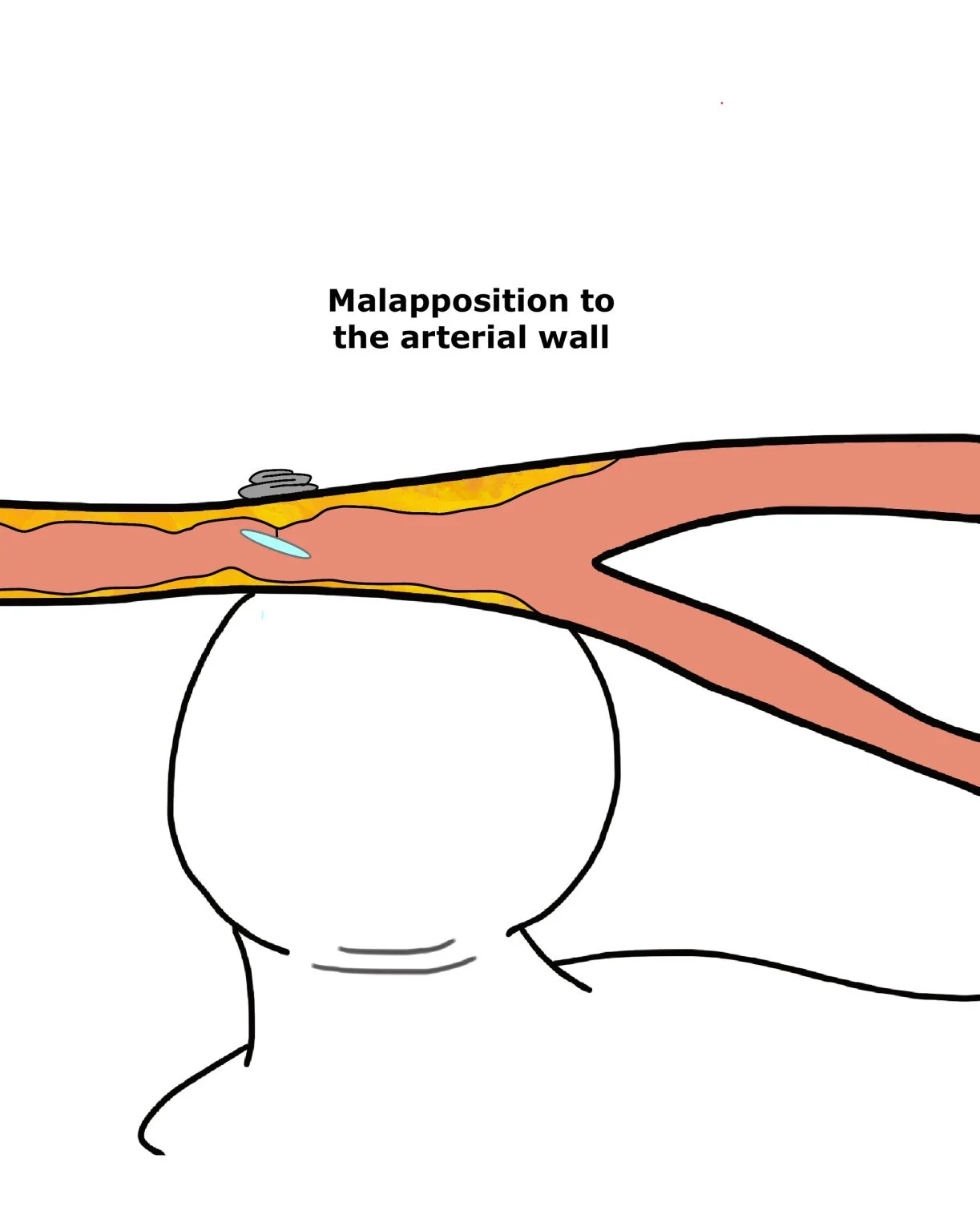
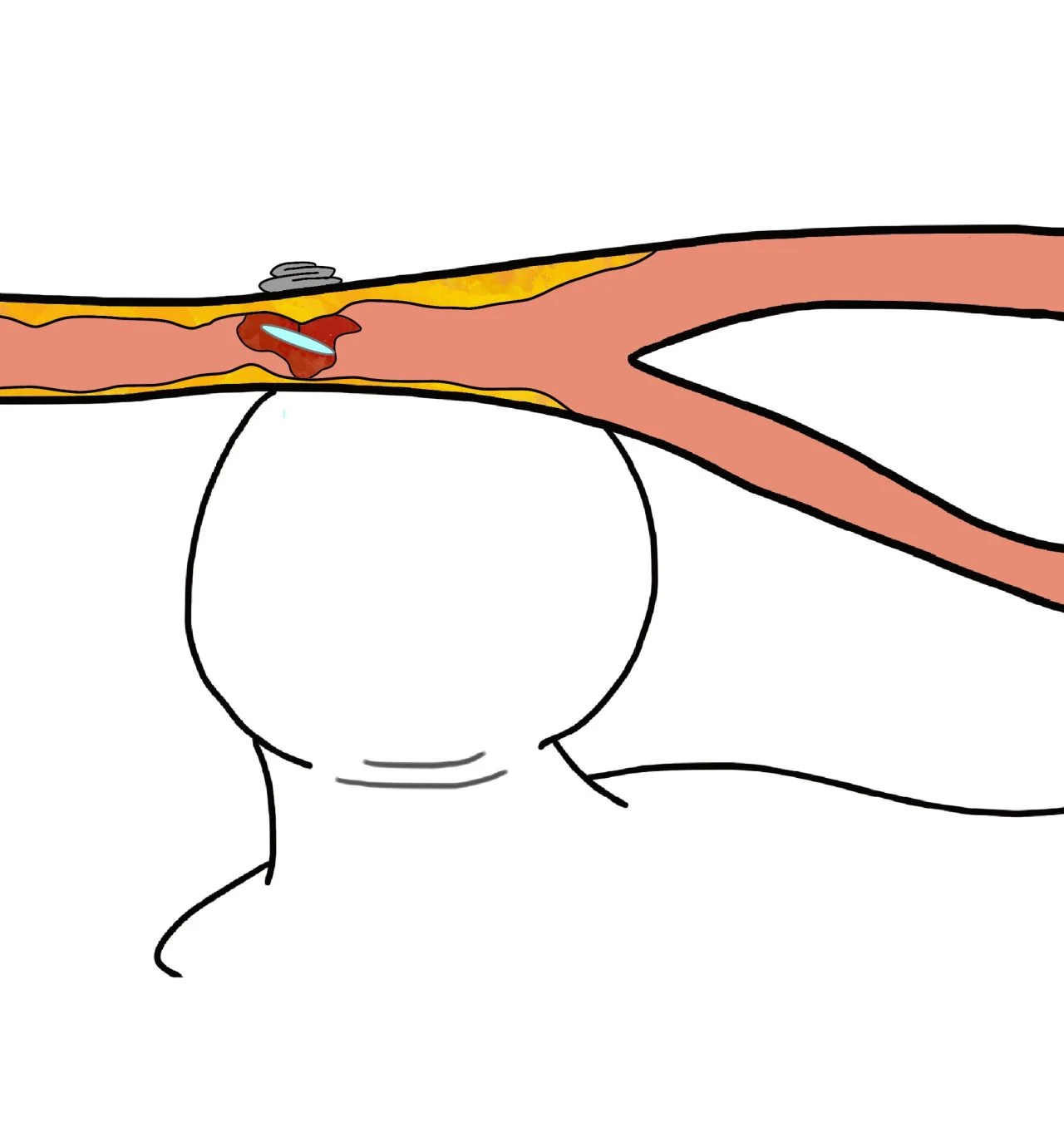
If you deploy a closure system that relies on proper wall apposition, and the device lands on a plaque, tension can be imperfect so the intraluminal component may end up malapposed.
And then two things can happen:
- Incomplete hemostasis is usually manageable with compression.
- The real problem: an intraluminal foreign body and disturbed flow can increase the risk of acute thrombosis/occlusion in a vessel you absolutely don’t want to lose.
So my practical rule is simple, but non-negotiable:
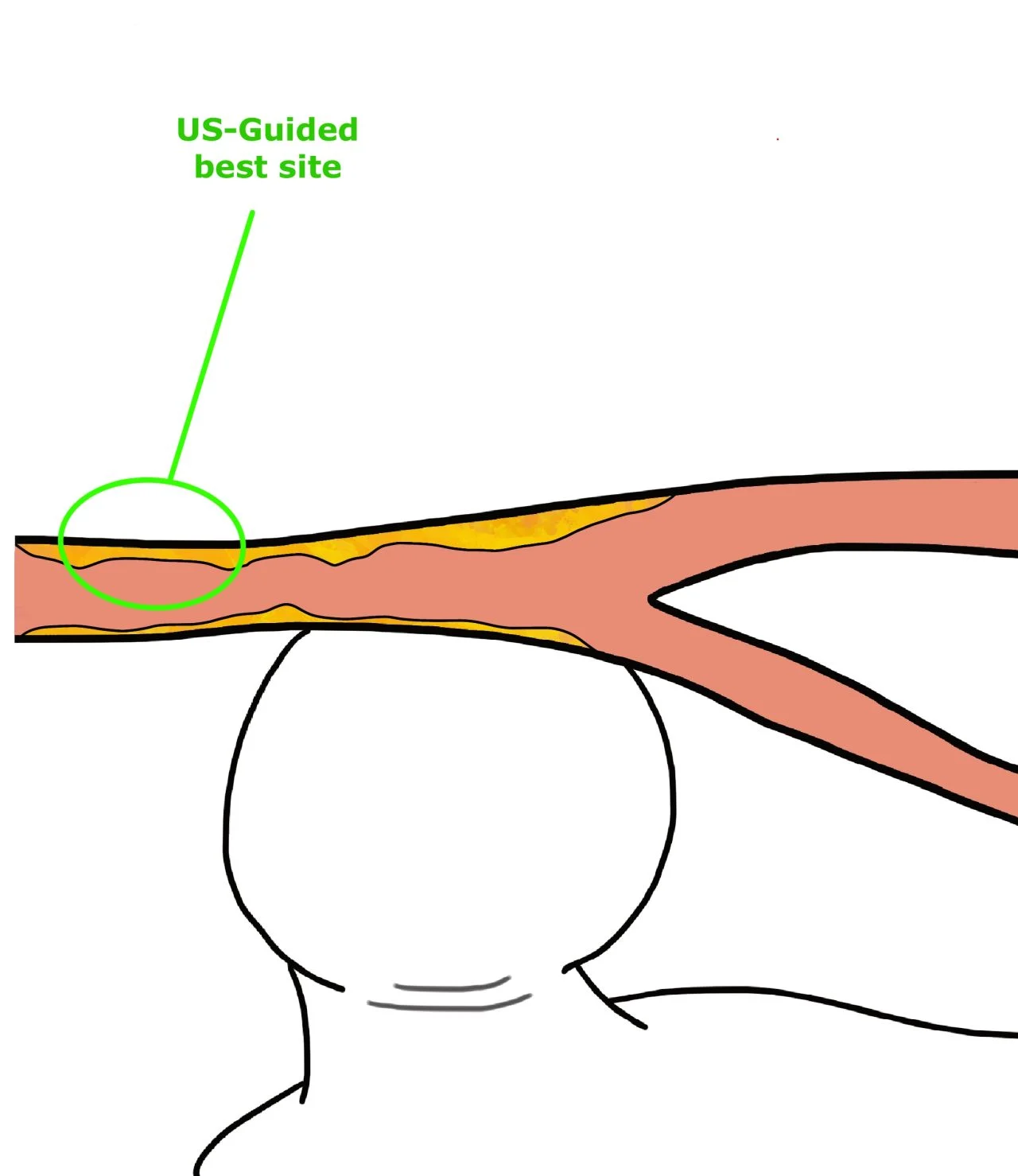
- US-guided puncture – always. Find the healthiest CFA segment.
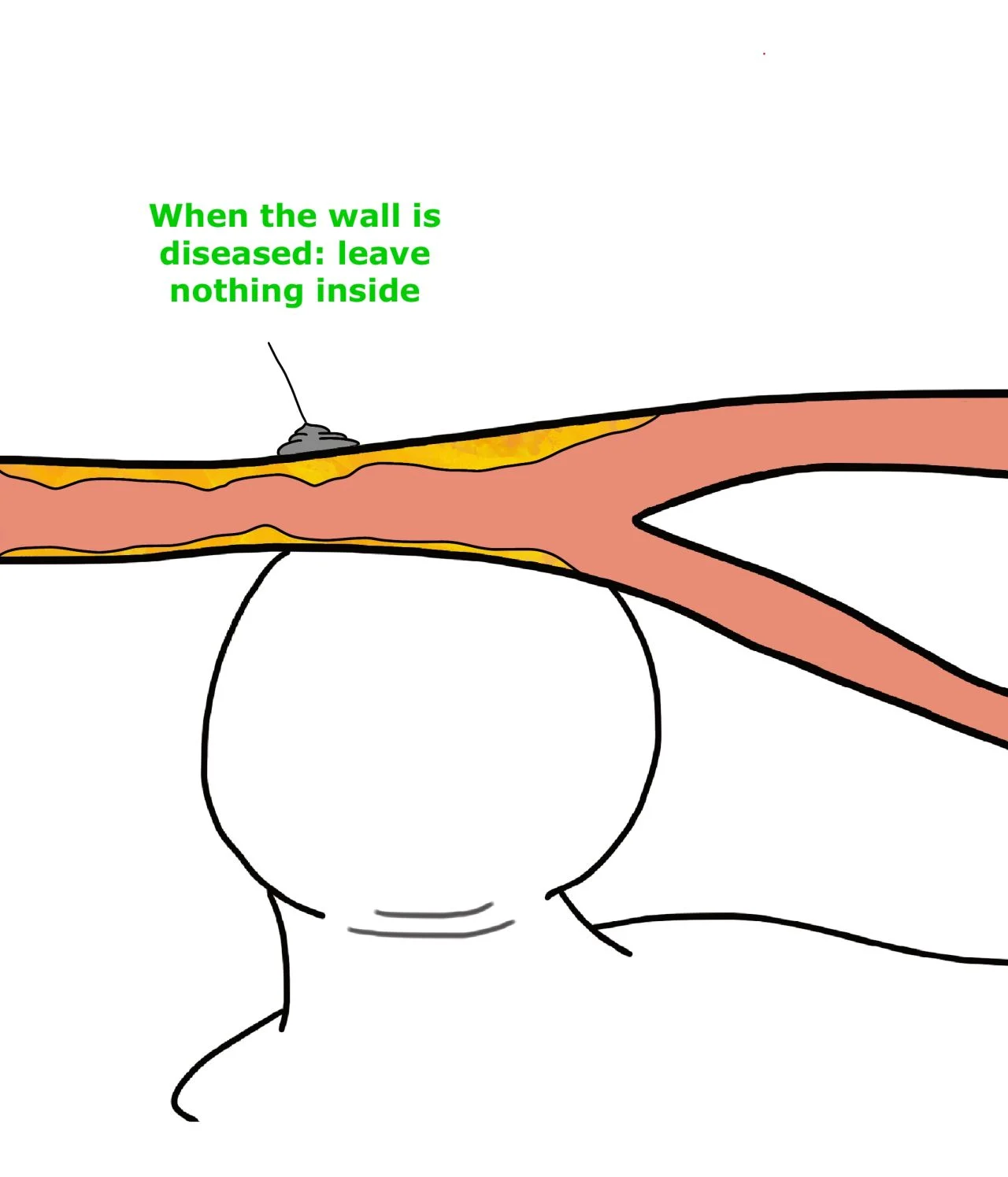
- If the wall is hostile and I can’t guarantee a safe landing zone, I’m happy to compress, or I choose a strategy that doesn’t leave anything intraluminal.
- Closure is not ‘after the case’. It’s part of the case.
How do you handle closure in a calcified / diseased CFA? Any personal red flags?”

Stay updated with Hemostasis Today.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-
Jun 26, 2026, 18:28Daniel Pereira Monteiro: Why Is Beta Thalassaemia Major so Severe?
-
Jun 26, 2026, 18:27Pradip Pawar: Cell and Gene Therapy – Transforming Medicine in the 21st Century
-
Jun 26, 2026, 18:26Aviva Schwartz: How Can We Better Protect Patients After an Ischemic Stroke?
-
Jun 26, 2026, 18:25Does Reversing Factor Xa Inhibitors Really Carry as Much Thrombotic Risk as We Think? – RPTH Journal
-
Jun 26, 2026, 18:25Akshat Jain: Novel Therapies in Childhood Blood and Cancer Disorders
-
Jun 26, 2026, 16:57Abdul Muqtadir Abbasi: Anticoagulation in DVT Patients With Hidden Varices Requires Extreme Caution
-
Jun 26, 2026, 16:42Anesa Mulabecirovic: Why Von Willebrand Disease Takes Years to Diagnose in Women
-
Jun 26, 2026, 16:32Kaitlin Lichty: A New Identity Reflecting a Shared Legacy of Bleeding Disorders
-
Jun 26, 2026, 16:07Toong Youttananukorn: The WFH Registry Driving Better Care and Advocacy