

Abdelrahman Essam: Why Early Hemorrhage Control Is Critical in Pelvic Fractures
Abdelrahman Essam, General Surgery and Trauma Doctor Specialist at Suez Medical Complex, shared a post on LinkedIn:
“A pelvic fracture doesn’t usually kill because of the broken bone.
It kills because of the bleeding you cannot see.
Pelvic fracture hemorrhage remains one of the most life-threatening emergencies in trauma surgery.
Although pelvic fractures account for a relatively small percentage of traumatic injuries, they are associated with some of the highest mortality rates when accompanied by massive hemorrhage.
The pelvis acts as a large potential space.
When disrupted by high-energy trauma, it can accommodate a significant volume of blood before obvious clinical signs appear.
By the time hypotension develops, the patient may have already lost a substantial amount of circulating blood.
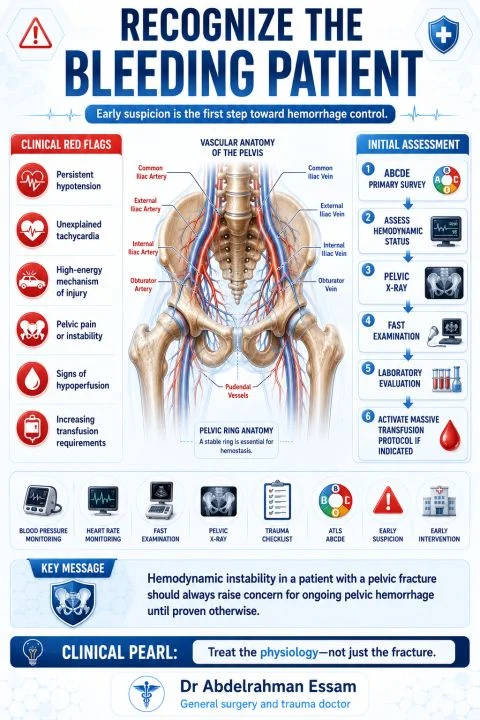
The first priority is not identifying the exact fracture pattern.
The first priority is recognizing the patient who is bleeding.
- Patients should immediately be assessed for:
- Hemodynamic instability
- High-energy mechanism of injury
- Signs of ongoing shock
- Pelvic instability when appropriate to assess
The majority of pelvic hemorrhage originates from venous bleeding and fractured cancellous bone surfaces, while a smaller proportion results from arterial injury.
This distinction is important because management strategies differ.
Early management follows a simple principle:
Reduce pelvic volume.
Restore physiology.
Control the bleeding.
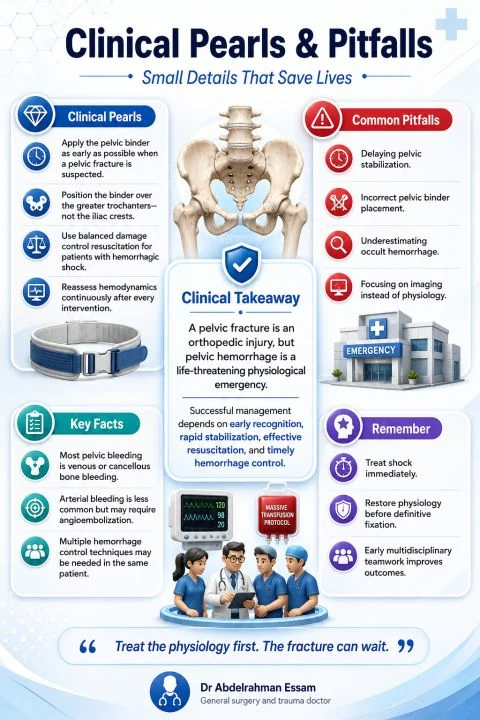
Applying a pelvic binder at the level of the greater trochanters is one of the fastest and most effective initial interventions.
Proper application stabilizes the pelvic ring, reduces pelvic volume, and may significantly decrease ongoing hemorrhage.
At the same time, balanced damage control resuscitation should begin immediately, including activation of a Massive Transfusion Protocol when indicated.
Definitive hemorrhage control depends on the patient’s physiology and available resources.
Options may include:
- Preperitoneal Pelvic Packing
- Angioembolization
- External pelvic fixation
These techniques are complementary—not competitive—and should be selected according to the clinical scenario.
Perhaps the greatest mistake is focusing solely on the fracture.
The fracture is only the injury.
Hemorrhage is the disease.
Clinical Takeaway
In pelvic trauma, don’t ask first, ‘How bad is the fracture?’
Ask instead,
‘Is this patient bleeding to death?’
That question saves lives.”

Stay updated with Hemostasis Today.
{kind=link}
{kind=link}
{kind=link}
-
Jul 2, 2026, 13:16Nathan Connell: Is It Time to Rethink What We Tell Hemophilia B Carriers About Pregnancy?
-
Jul 2, 2026, 13:09Bruce Ovbiagele: WSO SCDKIDS Task Force’s Webinar Sheds Light On Care of Sickle Cell Disease-Related Stroke
-
Jul 2, 2026, 12:55Taraneh G. Farazi: The Latest Stroke Clinician Issue Highlights the Importance of Patient Voices in Dysphagia Care
-
Jul 2, 2026, 12:45Kaveh Mehrvar: The Gut–Brain Axis May Hold New Clues to Stroke Pathophysiology
-
Jul 2, 2026, 12:28Expanding Stroke Education Through Mobile Stroke Clinics – Ethiopia Stroke Foundation
-
Jul 2, 2026, 11:52Praveen Kumar Tirlangi: A New Mechanism of Bleeding in Kyasanur Forest Disease
-
Jul 2, 2026, 11:17Heghine Khachatryan: Novel Biomarkers for Cancer-Associated Thrombosis
-
Jul 2, 2026, 11:17Neeraj Jain: Maharashtra Is Setting the Pace for Integrated Hemoglobinopathy Care
-
Jul 2, 2026, 11:11Safaa Hilal: Improving Postpartum Hemorrhage Outcomes Through Early Warning Scores