
Tagreed Alkaltham: WB Donation vs Apheresis Donation – Understanding Donor Reactions and Why They Differ
Tagreed Alkaltham, Transfusion Medicine Lab Supervisor at KSMC, shared a post on LinkedIn:
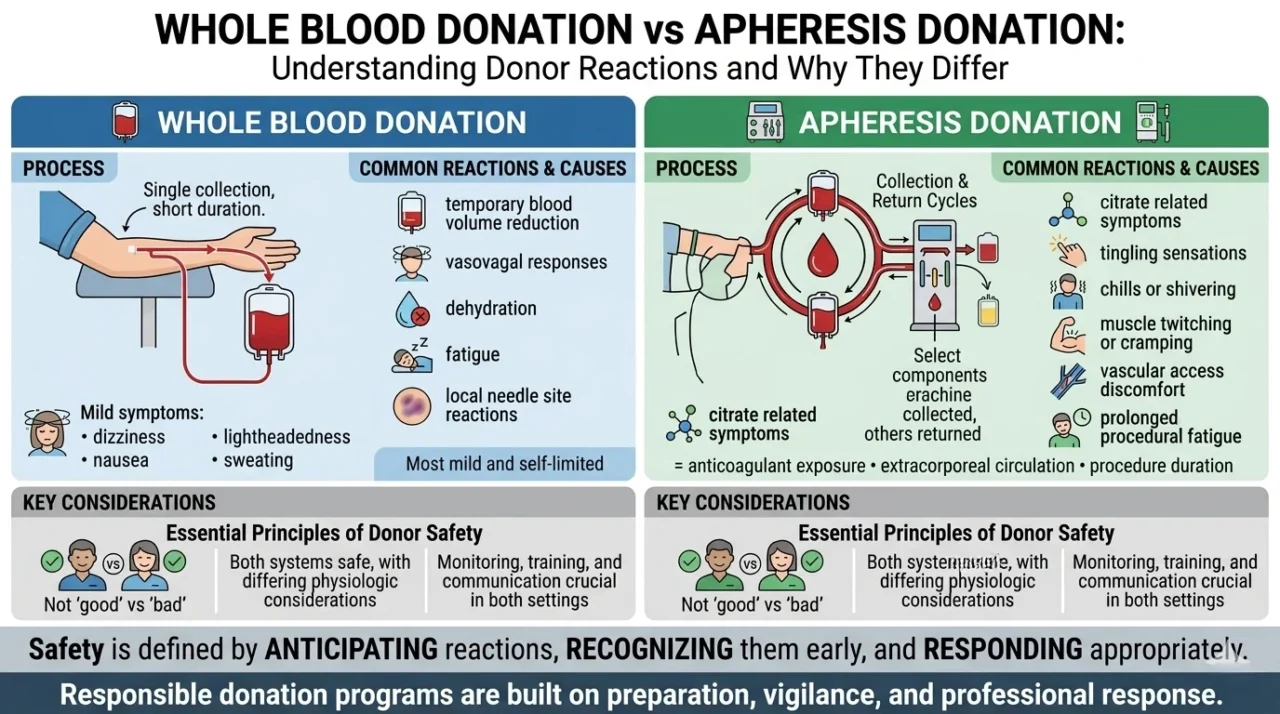
“Whole Blood Donation vs Apheresis Donation
Understanding Donor Reactions and Why They Differ
Not all donation reactions happen for the same reason. And not all donation procedures affect the body in the same way. That distinction matters.
Because whole blood donation and apheresis donation are fundamentally different processes physiologically, even though both are performed within structured donor safety systems.
In whole blood donation:
A unit of blood is collected directly from the donor over a relatively short period of time.
The most common donor reactions are often related to:
- temporary blood volume reduction
- vasovagal responses
- dehydration
- fatigue
- or local needle site reactions such as bruising
Some donors may experience:
- dizziness
- lightheadedness
- nausea
- sweating
- temporary weakness
Most reactions are mild and self limited.
In apheresis donation:
Blood continuously circulates through an extracorporeal circuit while selected components are collected and the remaining components are returned to the donor.
Because the procedure is different, the physiologic considerations are also different.
Apheresis reactions may involve:
- citrate related symptoms
- tingling sensations
- chills or shivering
- muscle twitching or cramping
- vascular access discomfort
- or prolonged procedural fatigue in some donors
These reactions are often associated with:
- anticoagulant exposure
- extracorporeal circulation
- procedure duration
- and continuous collection return cycles.
This does not mean one procedure is ‘good’ and the other is ‘bad.’
And it does not mean one donor reaction profile automatically makes one approach universally safer than the other. Each procedure has different physiologic considerations, monitoring priorities, and donor suitability requirements.
That is why donor selection, procedural monitoring, staff training, and communication remain essential in both settings.
The most important principle is this:
Safety in donation is not defined by the complete absence of physiologic reactions.
It is defined by:
- anticipating reactions
- recognizing them early
- responding appropriately
- and continuously improving donor care systems.
Because responsible donation programs are not built on perfect physiology. They are built on preparation, vigilance, and professional response.
The safest donation process is not the one with zero physiologic impact. It is the one where donor reactions are understood, monitored, and managed appropriately.”

Other posts featuring Tagreed Alkaltham on Hemostasis Today.
-
Aug 11, 2026, 08:20Hasan Abbas Zaheer: Strengthening Universal Access to Safe Blood in Pakistan
-
Aug 11, 2026, 08:07Nicola Pozzi: Advancing Hemostasis Through Scientific Collaboration at Hemostasis GRC
-
Aug 11, 2026, 07:50When Access to Care Changes Everything – WFH
-
Aug 11, 2026, 07:41Kevin Land: How Cellular Therapy Is Changing Transfusion Medicine
-
Aug 11, 2026, 07:35Kuldeep Singh Bhadauria: Building the Future of Hemophilia Care in India
-
Aug 11, 2026, 07:28Archil Jaliashvili: When Every Minute Matters Time Becomes a Therapy
-
Aug 11, 2026, 07:05Mavis Agnes Kisakye: Building Sustainable Transition Pathways in Hemophilia Care
-
Aug 11, 2026, 06:48Rishdha Roshad: What Happens to the Brain During Cardiopulmonary Bypass?
-
Aug 11, 2026, 05:53Isaac Okello: Strengthening Sickle Cell Advocacy in Uganda