

Abdulrahman Nasiri: Significant Shifts In The 2026 AHA/ACC Guidelines for Acute Pulmonary Embolism
Abdulrahman Nasiri, Assistant Professor of Medicine and Hematology at Imam Mohammad Ibn Saud Islamic University, shared on LinkedIn about the new AHA/ACC guideline by Mark A. Creager et al, adding:
“Major Clinical Update: The 2026 AHA/ACC Guidelines for Acute Pulmonary Embolism
For my colleagues in Hematology, Internal Medicine, and Cardiology, the newly released 2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guidelines for the Management of Acute Pulmonary Embolism introduce significant shifts that directly impact our daily clinical decision-making and patient protocols.
Here are the top takeaways:
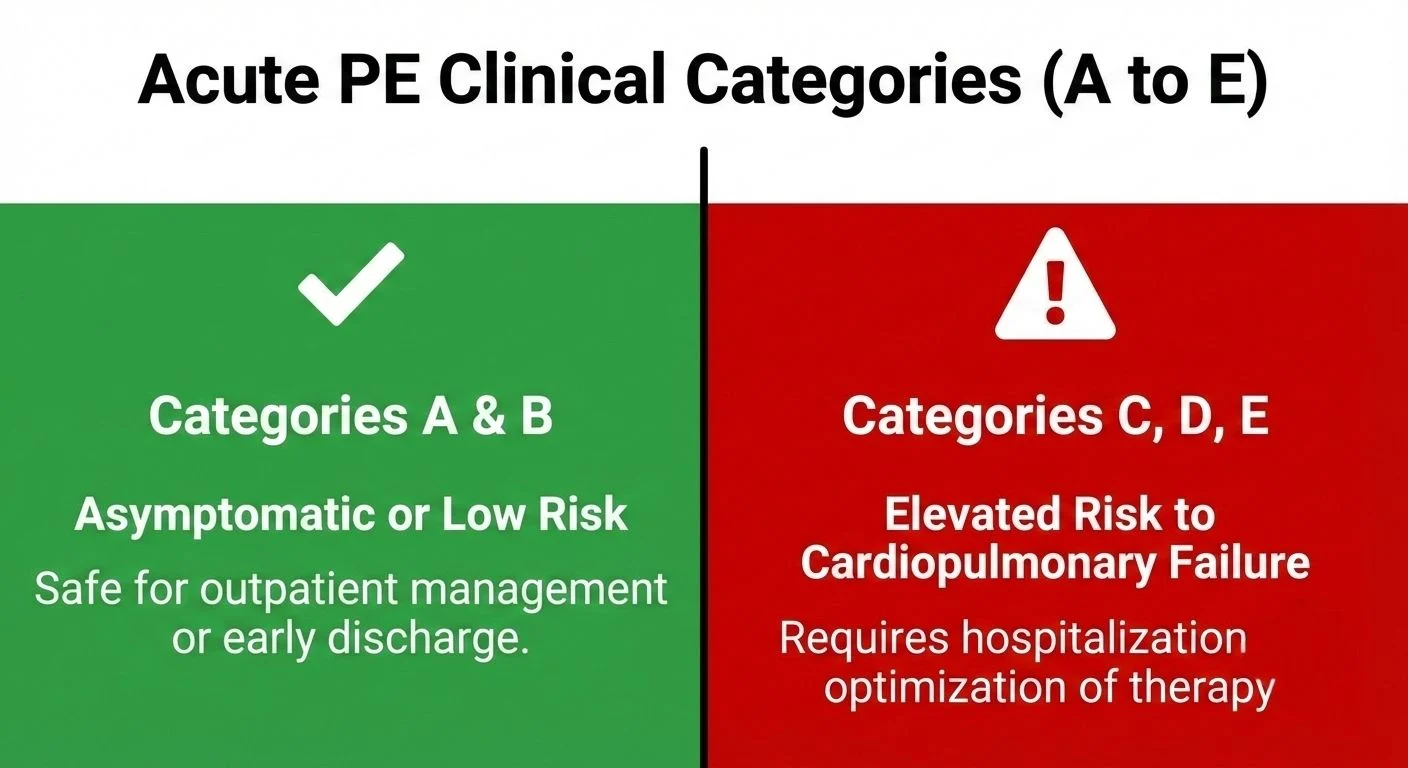
1. A New Era of Risk Stratification (Categories A-E)
Move over, simple ‘massive/submassive.’ The guidelines introduce a precise 5-tier Acute PE Clinical Categories system.
This integrates hemodynamics, biomarkers, and RV imaging to clearly delineate patients safe for outpatient management (Categories A and B) from those requiring hospitalization and potential advanced therapies (Categories C, D, E).
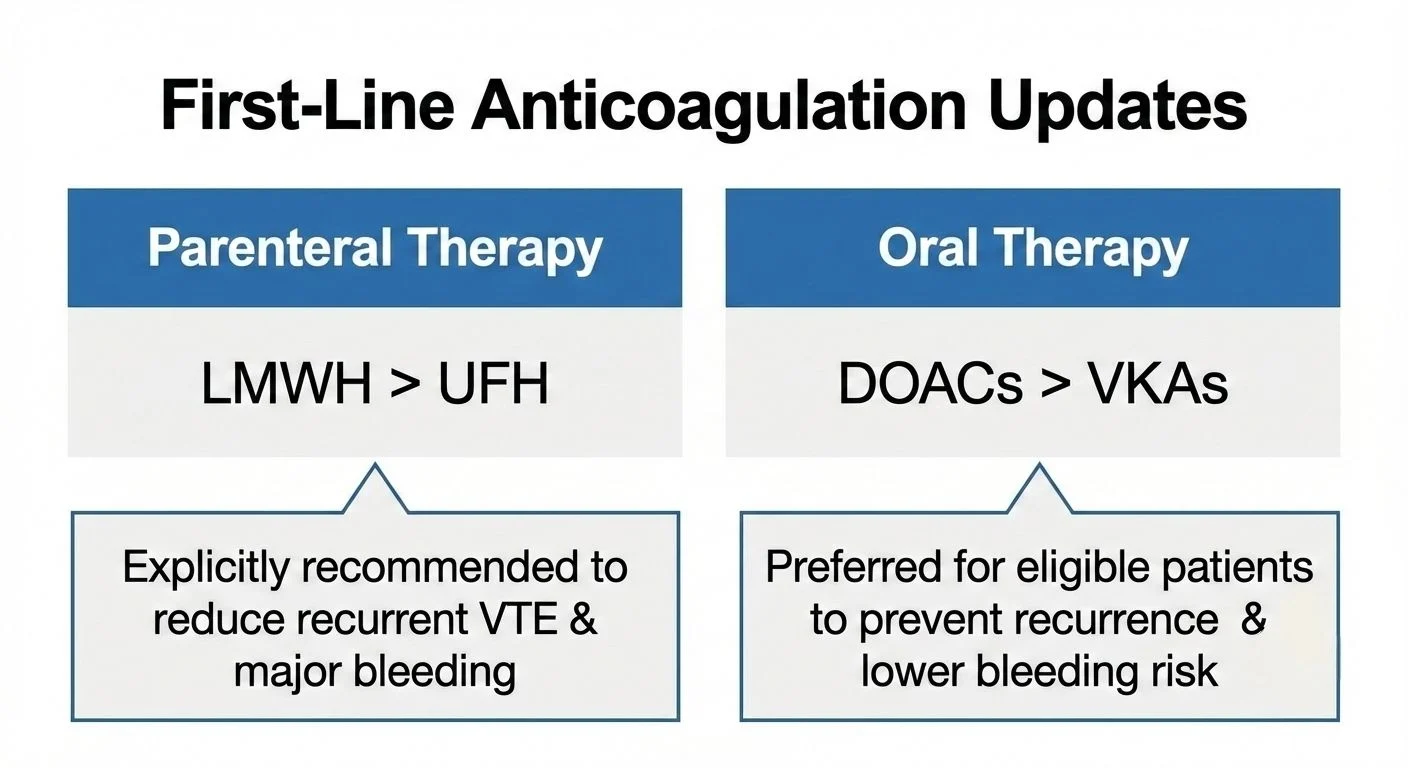
2. Anticoagulation Shifts (Crucial for Hematology)
- Oral: Direct Oral Anticoagulants (DOACs) are now unequivocally preferred over VKAs for eligible patients to prevent recurrence and reduce bleeding risk.
- Parenteral: When initial parenteral therapy is needed, Low-Molecular-Weight Heparin (LMWH) is explicitly recommended over UFH.
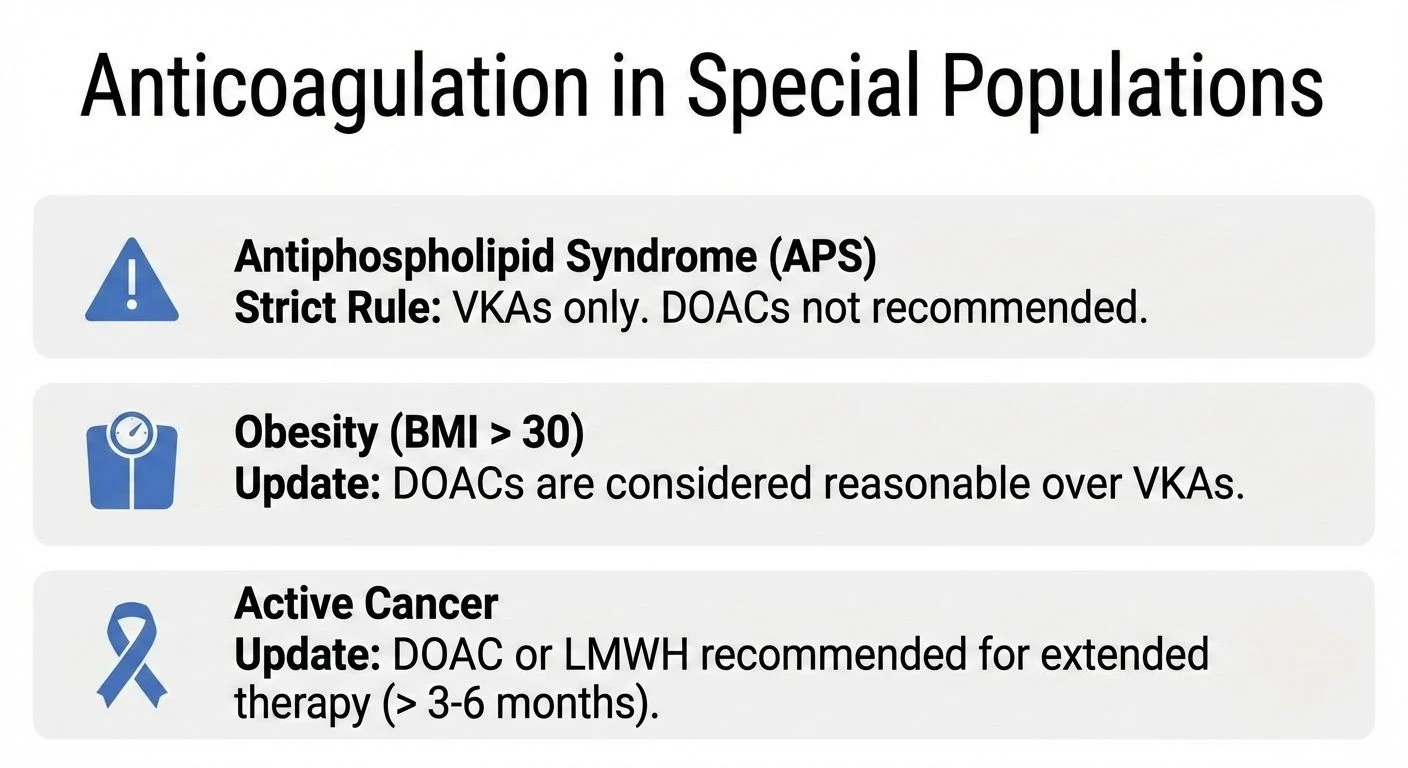
3. Special Populations Demand Specific Strategies.
The guidelines provide sharp clarity on complex cases:
- Antiphospholipid Syndrome (APS): A strict recommendation remains: VKAs only. DOACs should be avoided.
- Obesity and Cancer: DOACs are now considered reasonable over VKAs for obese patients (BMI >30) and are recommended alongside LMWH for extended cancer-associated thrombosis treatment.
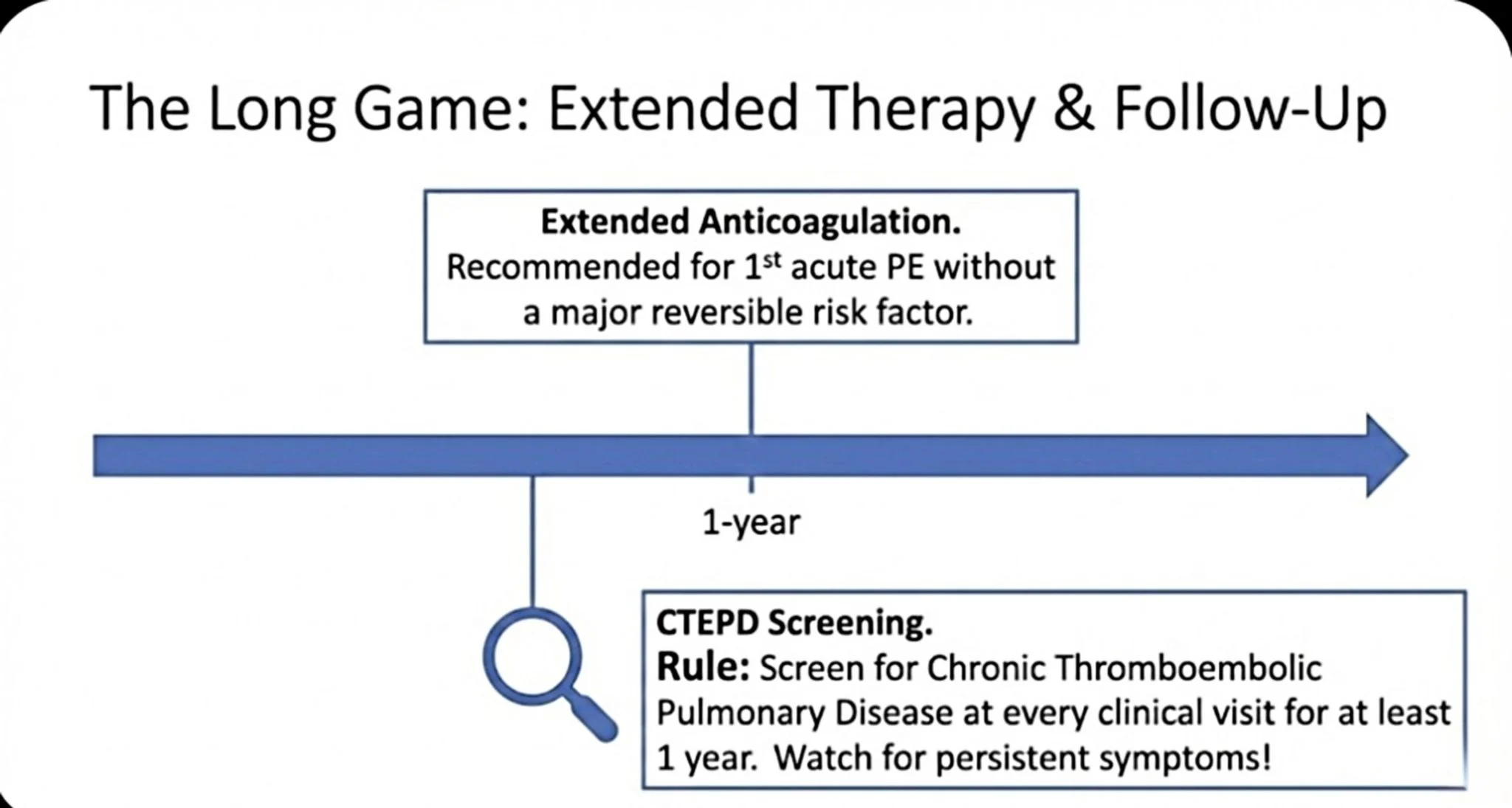
4. The ‘Long Game’ and CTEPD Screening
The job isn’t done at discharge.
Extended anticoagulation is recommended for unprovoked first PE.
Crucially, we must screen for Chronic Thromboembolic Pulmonary Disease (CTEPD) at every clinical visit for at least one year post-PE.
5. Systems of Care
The standard of care is now multidisciplinary.
The implementation of PE Response Teams (PERTs) is highly recommended to ensure timely, risk-stratified interventions for high-risk patients.
Swipe through the slides below for a visual summary of these key updates.
These changes represent a significant move toward more personalized, risk-adapted thrombosis care.”
Title: 2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines
Authors: Mark A. Creager, Geoffrey D. Barnes, Jay Giri, Debabrata Mukherjee, William Schuyler Jones, Allison E. Burnett, Teresa Carman, Ana I. Casanegra, Lana A. Castellucci, Sherrell M. Clark, Mary Cushman, Kerstin de Wit, Jennifer M. Eaves, Margaret C. Fang, Joshua B. Goldberg, Stanislav Henkin, Hillary Johnston-Cox, Sabeeda Kadavath, Daniella Kadian-Dodov, William Brent Keeling, Andrew J. P. Klein, Jun Li, Michael C. McDaniel, Lisa K. Moores, Gregory Piazza, Karen S. Prenger, Steven C. Pugliese, Mona Ranade, Rachel P. Rosovsky, Farla Russo, Eric A. Secemsky, Akhilesh K. Sista, Leben Tefera, Ido Weinberg, Lauren M. Westafer, Michael N. Young
Read the Full Article on Circulation

Stay updated on all scientific advances with Hemostasis Today.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-
Jul 5, 2026, 18:58Linda Hayes Bennett: Redefining Ferroptosis in Aging and Neurodegenerative Conditions
-
Jul 5, 2026, 18:20LV Aneurysm, Thrombus, and Embolism: A Silent Post-MI Threat – Abdallah Othman
-
Jul 5, 2026, 17:58Andaleb Kholmukhamedov: What’s the Most Unusual “False Positive” Trigger You’ve Seen Elevate a D-Dimer?
-
Jul 5, 2026, 17:47Michiel Coppens: Supporting Better Hemophilia Care in Suriname
-
Jul 5, 2026, 17:31Arrigo Francesco Giuseppe Cicero: Redefining the Role of Urate-Lowering Therapy in Cardiovascular Disease
-
Jul 5, 2026, 17:20Ahmad Gharehbaghian: Iranian Blood Transfusion Organization Engages Government Leaders on Blood Service Investment
-
Jul 5, 2026, 17:03Paolo Zamboni։ New Findings Highlight PLXND1 as a Critical Mechanosensor in Primary Lymphedema
-
Jul 5, 2026, 16:42Marta Sobas: Advancing Pregnancy Care in Myeloproliferative Neoplasms in IHEM
-
Jul 5, 2026, 15:19Marc Carrier: Celebrating 25 Years of Excellence in Thrombosis Training at ISTH 2026