

Georges Chahoud: Top Take-Home Messages from the AHA/ACC/Multisociety Acute PE Guideline
Georges Chahoud, Heart Failure Cardiologist at St. Louis Cardiology, shared a post on LinkedIn:
“The following Top Take-Home Messages are taken directly from the AHA/ACC/Multisociety Acute PE Guideline.
1 Messages 1, 5, and 6 (in bold below) were selected as key themes by the ACC Acute PE Guideline Dissemination Workgroup for this Guideline-at-a-Glance as they represent the most impactful changes and address established gaps in clinical practice.
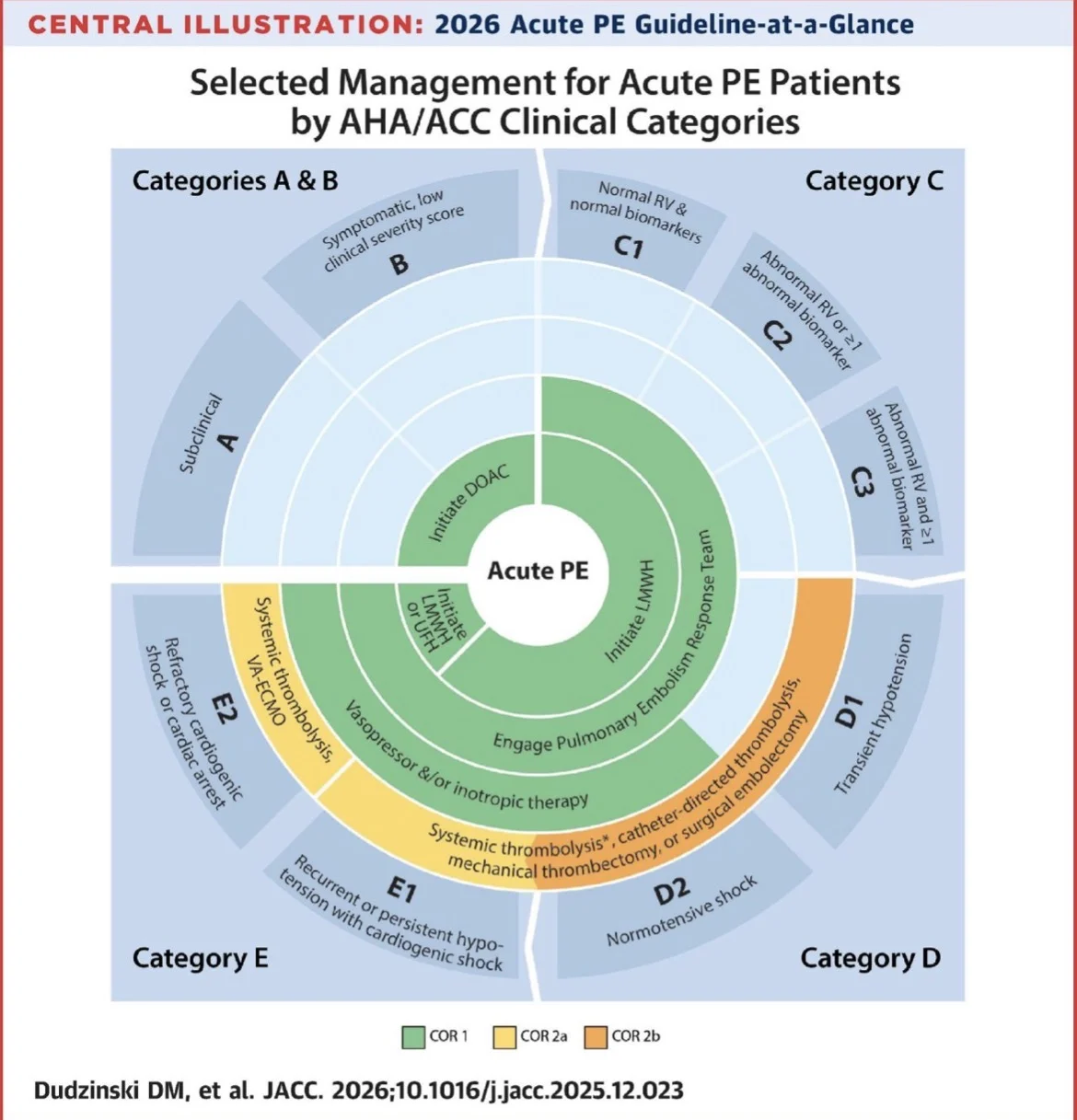
1. A new clinical classification scheme is presented, entitled “Acute Pulmonary Embolism Clinical Categories,” with 5 categories (A-E) and subcategories, ranging from low to high risk for adverse outcomes, in order to enhance the precision of severity classification, prognosis assessment, and evidence-based therapeutic decision-making for patients presenting with acute PE.
2. Patients with acute PE who are asymptomatic (AHA/ACC PE Category A) can safely be discharged home from the emergency room and do not need to be hospitalized.
3. Early hospital discharge is generally recommended for patients with acute PE who are symptomatic but have a low clinical severity score (AHA/ACC PE Category B).
4. Symptomatic patients with acute PE and an elevated clinical severity score, including those with elevated biomarkers and/or right ventricular dysfunction (AHA/ACC PE Category C), incipient cardiopulmonary failure (AHA/ACC PE Category D), and those with cardiopulmonary failure characterized by persistent hypotension (AHA/ACC PE Category E) should be hospitalized to optimize treatment strategies.
5. Advanced therapies, including systemic thrombolysis, catheter-based thrombolysis, mechanical thrombectomy, and surgical embolectomy are reasonable for patients with acute PE in AHA/ACC PE Category E1 and can be considered for patients with acute PE in AHA/ACC PE Category D1-2.
6. PE response teams (PERTs) are recommended to improve timeliness of care.
7. In patients with acute PE who require initial parenteral anticoagulant therapy, low-molecular-weight heparin is recommended over unfractionated heparin.
8. In patients with acute PE who are eligible for oral anticoagulation, direct oral anticoagulants are recommended over vitamin K antagonists, unless contraindicated, to prevent recurrent venous thromboembolism and reduce major bleeding.
9. In patients with a first acute PE without a major reversible risk factor and in those with a persistent risk factor, continuing anticoagulation beyond the initial treatment phase (3-6 months) into the extended phase is recommended.
10. Patients who have had acute PE should be asked about PE-related symptoms and functional limitations at every visit for at least 1 year to screen for chronic thromboembolic pulmonary disease or other causes of dyspnea and functional limitation.”
American College of Cardiology shared a post on LinkedIn:
“The 2026 ACC/AHA/Multisociety Clinical Guideline on acute pulmonary embolism focuses on evaluation, management, and follow-up of adult patients.
This Guideline-at-a-Glance highlights practice-changing recommendations from the guideline to accelerate adoption.”
Title: 2026 Acute Pulmonary Embolism Guideline-at-a-Glance
Authors: David M. Dudzinski, Morgane Cibotti-Sun, Mykela M. Moore
Read the Full Article on JACC Journals

Stay updated on all scientific advances with Hemostasis Today.
{kind=link}
-
Jun 29, 2026, 06:48Christina Pohlman: Anticoagulants and Bone Health – APS Awareness Month Day 23
-
Jun 29, 2026, 06:33Andreas Calatzis: Can Fibrinolysis Sensitivity Be Claimed Without a Reference Standard
-
Jun 29, 2026, 06:25Aliaa Albadri: When a Hair Wash Leads to a Stroke Workup
-
Jun 29, 2026, 06:22Tehreen Parveen: Historical Milestone in Drug Discovery – The Discovery of Aspirin
-
Jun 29, 2026, 06:16Muhammad Sufyan: Deep Vein Thrombosis – Recognizing the Warning Signs
-
Jun 29, 2026, 05:33Janak Sadhu: Uniting for The Stroke-Free Mehsana Initiative
-
Jun 29, 2026, 05:20Deepti Sachan: A Global Exchange Shaping the Future of Transfusion Medicine at ISBT 2026
-
Jun 29, 2026, 04:50Scott Cameron: ACC/AHA Guidance on Acute Pulmonary Embolism Management
-
Jun 29, 2026, 03:10Aryabhatta Sadhu: ABO and Rh Incompatibility In Stem Cell Transplantation