

Rola Fayad Shares Key Clinical Updates on Anemia in CKD from KDIGO 2026
Rola Fayad, Nephrologist at HHUMC, shared on LinkedIn:
‘‘KDIGO 2026 Anemia in CKD: Key Clinical Updates!
The new KDIGO 2026 Guideline for Anemia in CKD offers clearer definitions, more precise thresholds, and a more patient‑centered approach to anemia management.
As nephrologists, these updates help us deliver safer and more individualized care.
Definition and Screening:
– Anemia: Hb <12 g/dL (women), <13 g/dL (men).
– Screening:
• G3: yearly
• G4: twice yearly
• G5/dialysis: every 3 months
Initial tests: CBC, reticulocytes, ferritin, TSAT.
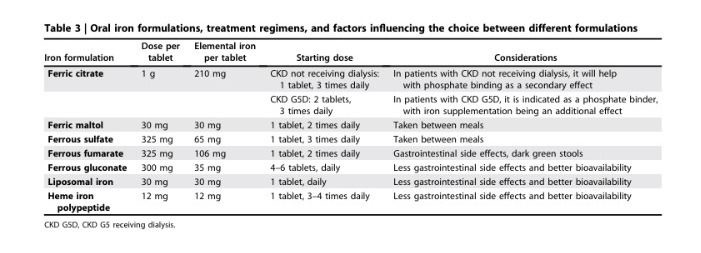
Updated Iron Concepts:
– Systemic iron deficiency: ferritin <100 ng/mL (ND) or <200 ng/mL (HD), TSAT <20%.
– Iron‑restricted erythropoiesis: ferritin >100–200 ng/mL with TSAT <20%.
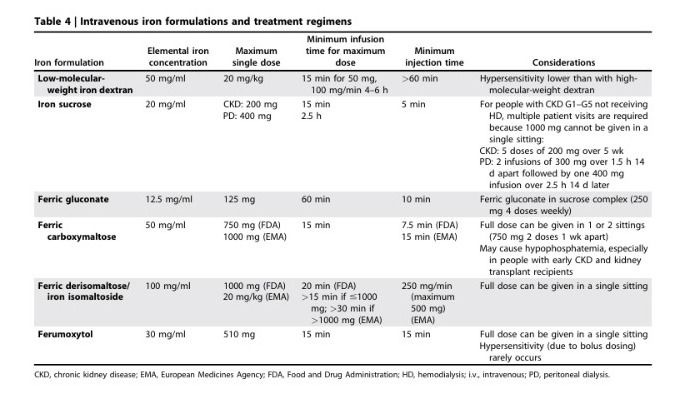
When to Start Iron Therapy:
– Hemodialysis:
• Start IV iron if ferritin ≤500 ng/mL and TSAT ≤30%.
• Withhold if ferritin >700 ng/mL or TSAT ≥40%.
– Non‑dialysis CKD:
• Ferritin <100 and TSAT <40%, or
• Ferritin 100–300 and TSAT <25%
– Oral or IV based on tolerance and response.
– Hold iron during active infection.
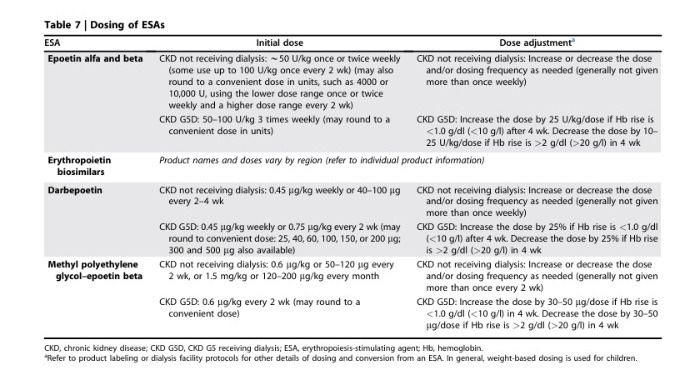
ESA Therapy:
– Dialysis: start when Hb ≤9–10 g/dL.
– Non‑dialysis: consider at Hb 8.5–10 g/dL based on symptoms.
– Do not maintain Hb ≥11.5 g/dL.
– Monitor Hb every 2–4 weeks.
– Suspend ESA during stroke or thrombosis; use caution in active malignancy.
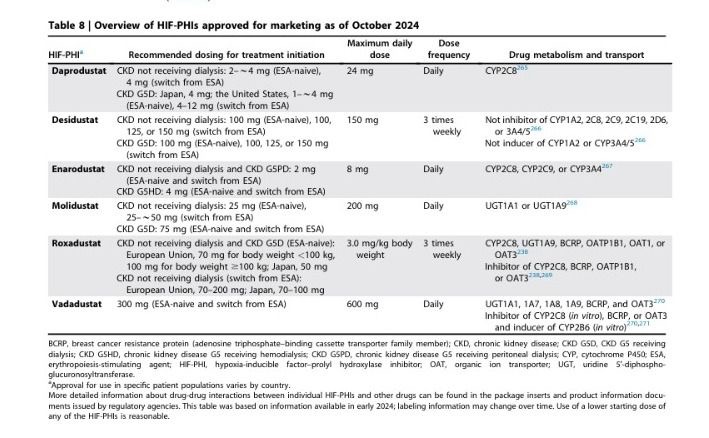
HIF‑PHIs:
– Option when ESA intolerance or hypo-responsiveness.
– Avoid in active malignancy, recent CV/thrombotic events, Pregnancy, Pulmonary hypertension, Proliferative retinal disease.
– Stop after 3–4 months if no response.
Transfusions:
– Reserved for acute or symptomatic or life‑threatening anemia.
-Avoid when possible in transplant candidates.
What I appreciate most about these guidelines is that they remind us of something essential: Anemia Management in CKD is not just about numbers it’s about people.
It’s about reducing fatigue, improving cognition, protecting the heart, and restoring dignity and quality of life.
These recommendations help us deliver care that is safer, more precise, and more compassionate.”

Stay updated with Hemostasis Today.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-
Jul 7, 2026, 23:20Balaji Balagani: Exploring Pulmonary Embolism
-
Jul 7, 2026, 23:03Roxana González Mazarío: The Phenotype-Specific Cardiovascular Risks in AAV
-
Jul 7, 2026, 22:52Harry Spoelstra: LongC0VID Still has Zero Proven Treatments
-
Jul 7, 2026, 22:39Satya K. Morar: Acute Portal Vein Thrombosis as an Exceptionally Rare Complication of Liver Biopsy in CVID
-
Jul 7, 2026, 22:23Aravind Palraj: Antiphospholipid Syndrome is not Just ‘Start Warfarin and Follow INR’
-
Jul 7, 2026, 20:59William Aird: An Unlucky Turn Into the Renal Artery
-
Jul 7, 2026, 20:58Chokri Ben Lamine: The Two-Hit Model of TRALI
-
Jul 7, 2026, 20:57New Issue of Blood Out Now – Blood Journals Portfolio
-
Jul 7, 2026, 20:56Priyadarshini Ramakrishnan: Schistocytes – The Most “Misleading Heroes” in a Peripheral Smear