

Bartosz Hudzik: High Bleeding Risk Does Not Always Mean Bleeding-Risk Predominance
Bartosz Hudzik, Associate Profesor at Medical University of Silesia, shared a post on LinkedIn:
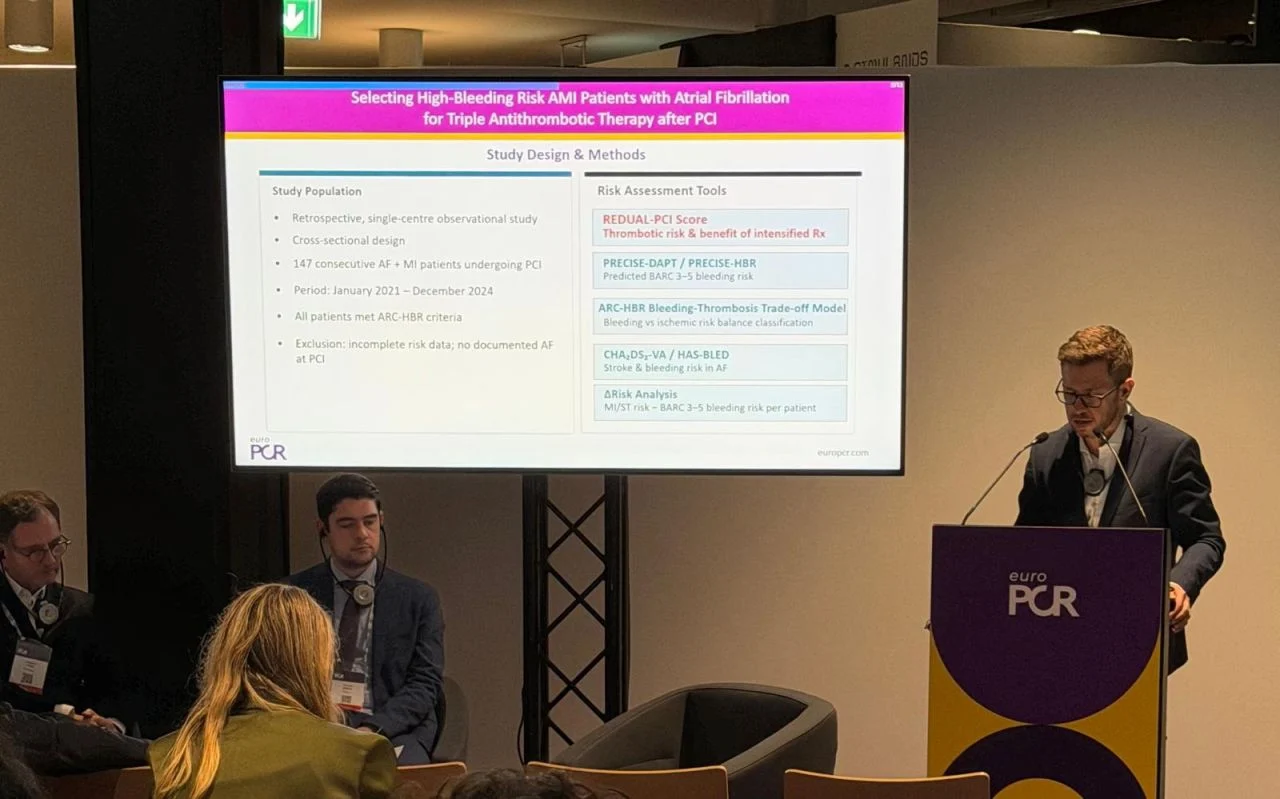
“At EuroPCR 2026, we are presenting our results:
‘Selecting high-bleeding risk AMI patients with AF for triple antithrombotic therapy after PCI‘
Contemporary antithrombotic management in AF-PCI patients has progressively shifted toward treatment de-escalation, largely driven by concerns surrounding bleeding.
Yet the prevailing paradigm that all high bleeding risk (HBR) patients should uniformly receive abbreviated or simplified regimens deserves reconsideration.
In our cohort of AF patients presenting with STEMI and NSTEMI undergoing PCI, integration of the REDUAL-PCI score with the ARC-HBR trade-off model identified a clinically relevant subgroup in whom ischemic risk remained predominant despite clear HBR features.
Key observations:
- More than 70% of patients demonstrated a REDUAL-PCI score ≥5
- These patients had substantially greater ischemic burden, including prior MI, CKD, and complex PCI
- Ischemic-dominant profiles were threefold more frequent among REDUAL ≥5 patients
- Estimated MI/stent thrombosis risk substantially exceeded bleeding liability in a significant proportion of HBR patients
The important message is straightforward:
High bleeding risk does not necessarily equate to bleeding-risk predominance.
A growing tendency exists to treat HBR as a therapeutic endpoint rather than as one component of a broader competing-risk equation.
Our data suggest this approach may oversimplify decision-making in AF-PCI patients, particularly in those with advanced atherosclerotic and thrombotic substrates.
The combination of REDUAL-PCI and ARC-HBR trade-off assessment may help identify patients in whom ischemic protection remains critically important and in whom triple antithrombotic therapy should not be dismissed reflexively.
The field likely needs to move beyond standardized de-escalation algorithms toward a more nuanced and personalized antithrombotic strategy — one based not solely on bleeding vulnerability, but on the dynamic balance between bleeding and thrombosis.”

Other posts featuring Bartosz Hudzik on Hemostasis Today.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-
Jul 7, 2026, 23:20Balaji Balagani: Exploring Pulmonary Embolism
-
Jul 7, 2026, 23:03Roxana González Mazarío: The Phenotype-Specific Cardiovascular Risks in AAV
-
Jul 7, 2026, 22:52Harry Spoelstra: LongC0VID Still has Zero Proven Treatments
-
Jul 7, 2026, 22:39Satya K. Morar: Acute Portal Vein Thrombosis as an Exceptionally Rare Complication of Liver Biopsy in CVID
-
Jul 7, 2026, 22:23Aravind Palraj: Antiphospholipid Syndrome is not Just ‘Start Warfarin and Follow INR’
-
Jul 7, 2026, 20:59William Aird: An Unlucky Turn Into the Renal Artery
-
Jul 7, 2026, 20:58Chokri Ben Lamine: The Two-Hit Model of TRALI
-
Jul 7, 2026, 20:57New Issue of Blood Out Now – Blood Journals Portfolio
-
Jul 7, 2026, 20:56Priyadarshini Ramakrishnan: Schistocytes – The Most “Misleading Heroes” in a Peripheral Smear