

Brandy Seyller: Why Understanding the Coagulation Cascade Matters in Bleeding Cases
Brandy Seyller, Founder of ClinicianExperts.com and MedLexHQ.com, shared a post on LinkedIn:
“If you don’t understand the coagulation cascade, you can’t evaluate a bleeding case for merit.
I mean that literally. Especially an ECMO case.
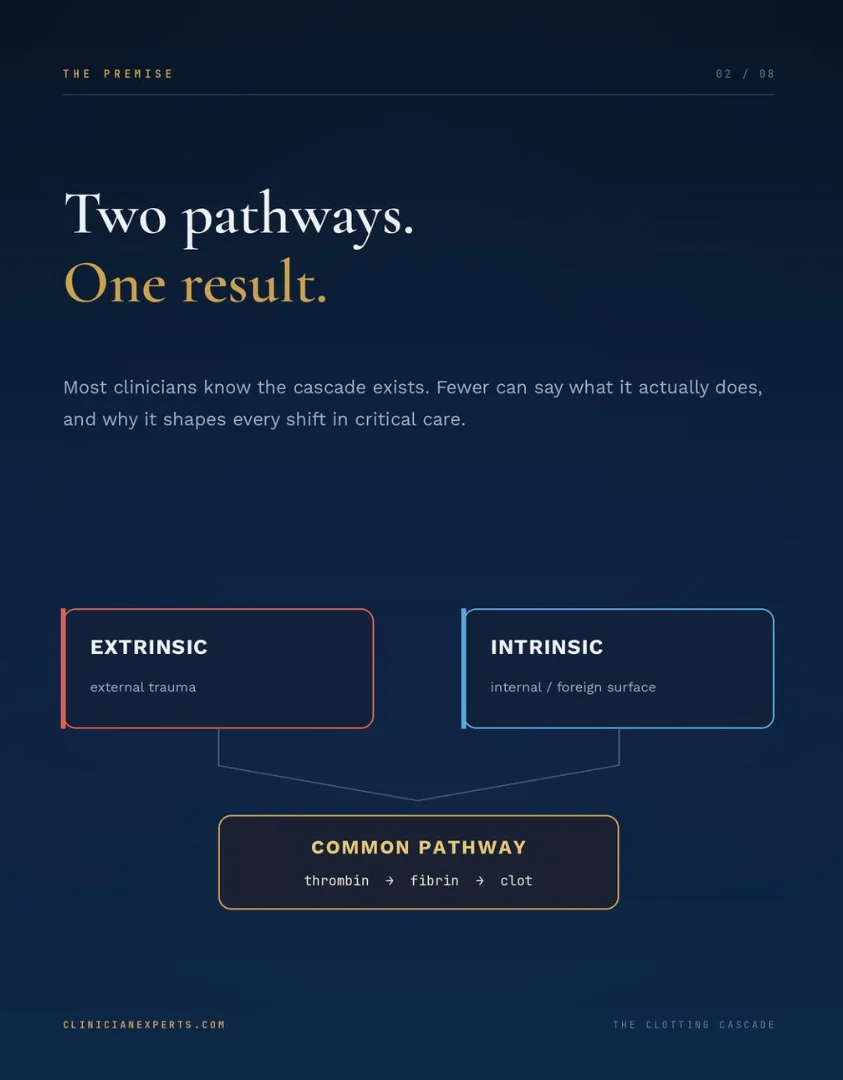
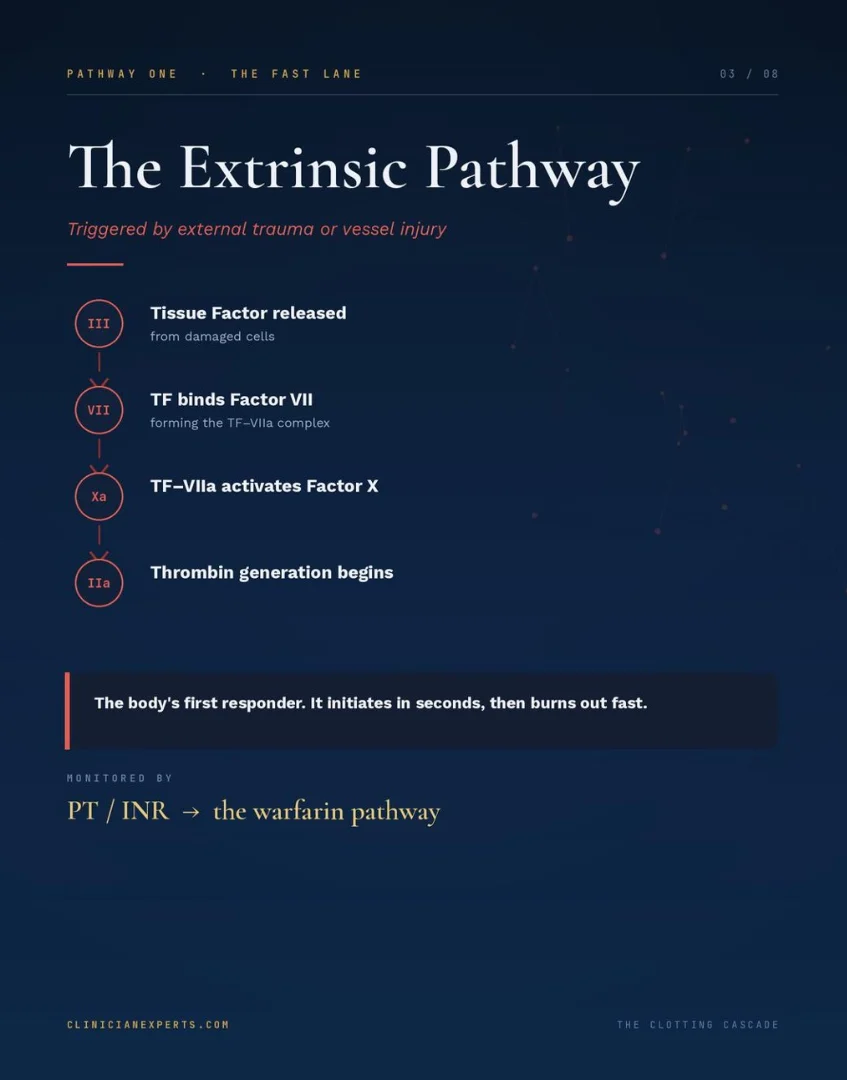
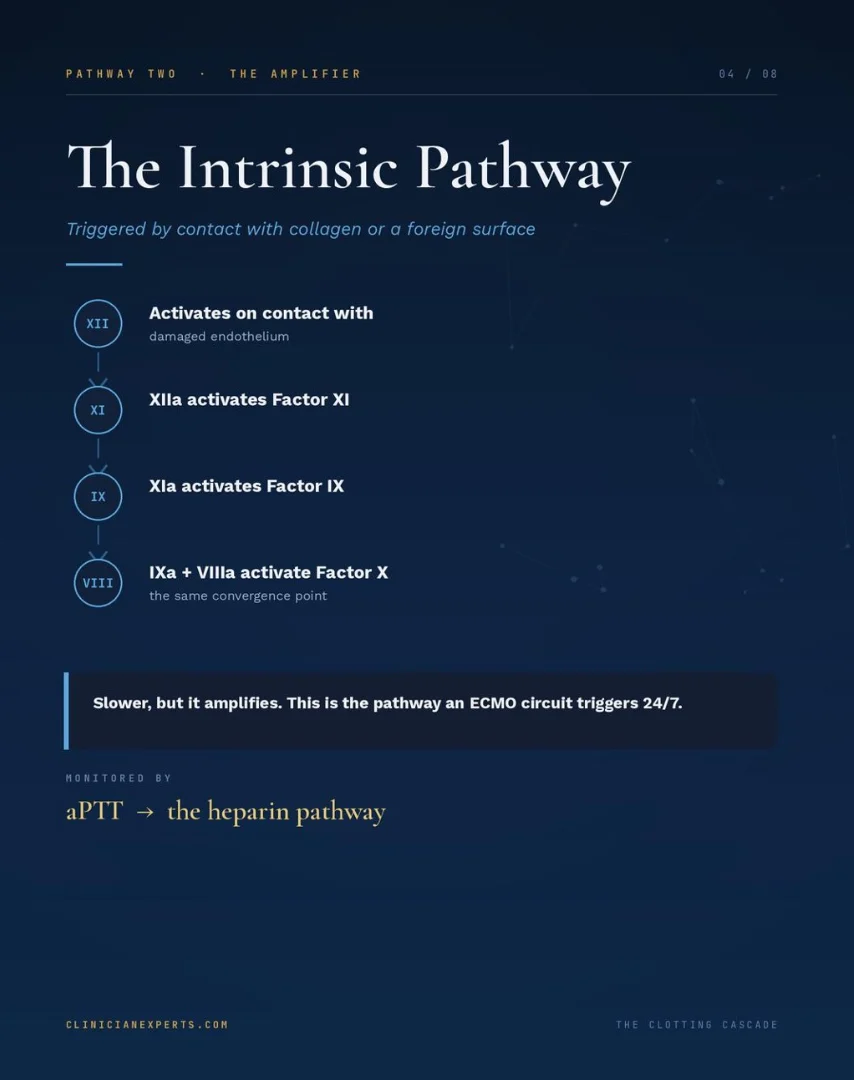
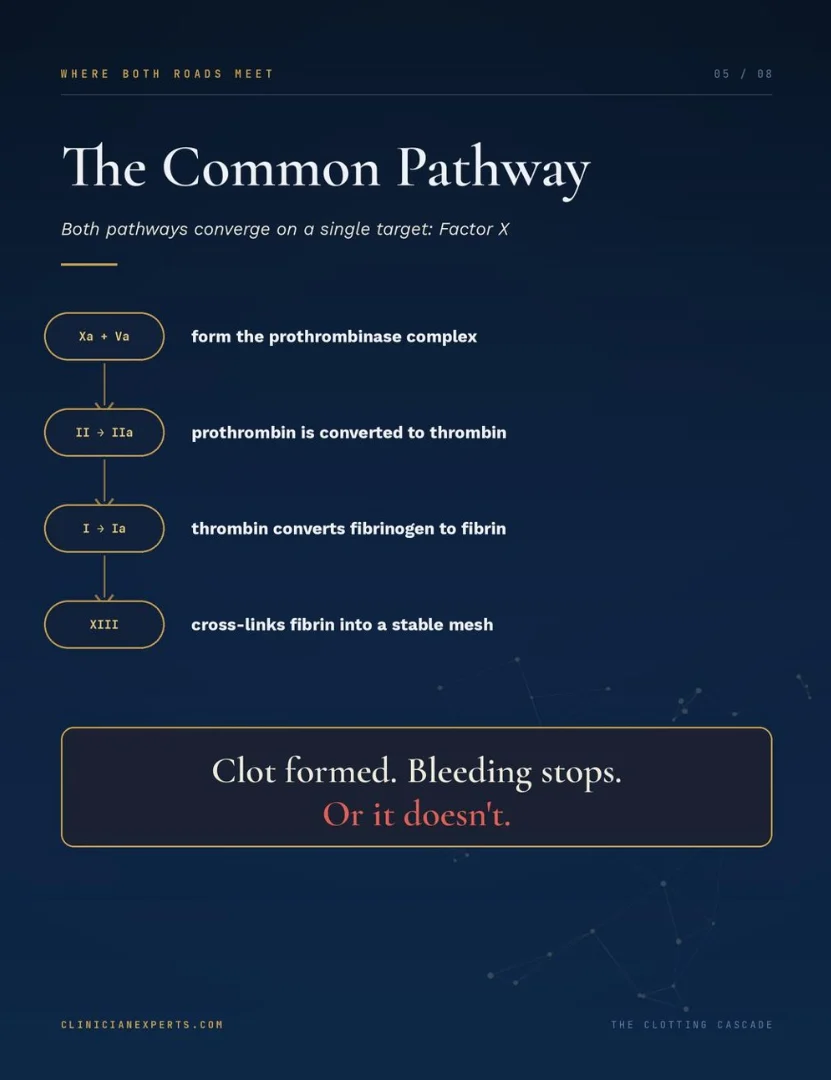
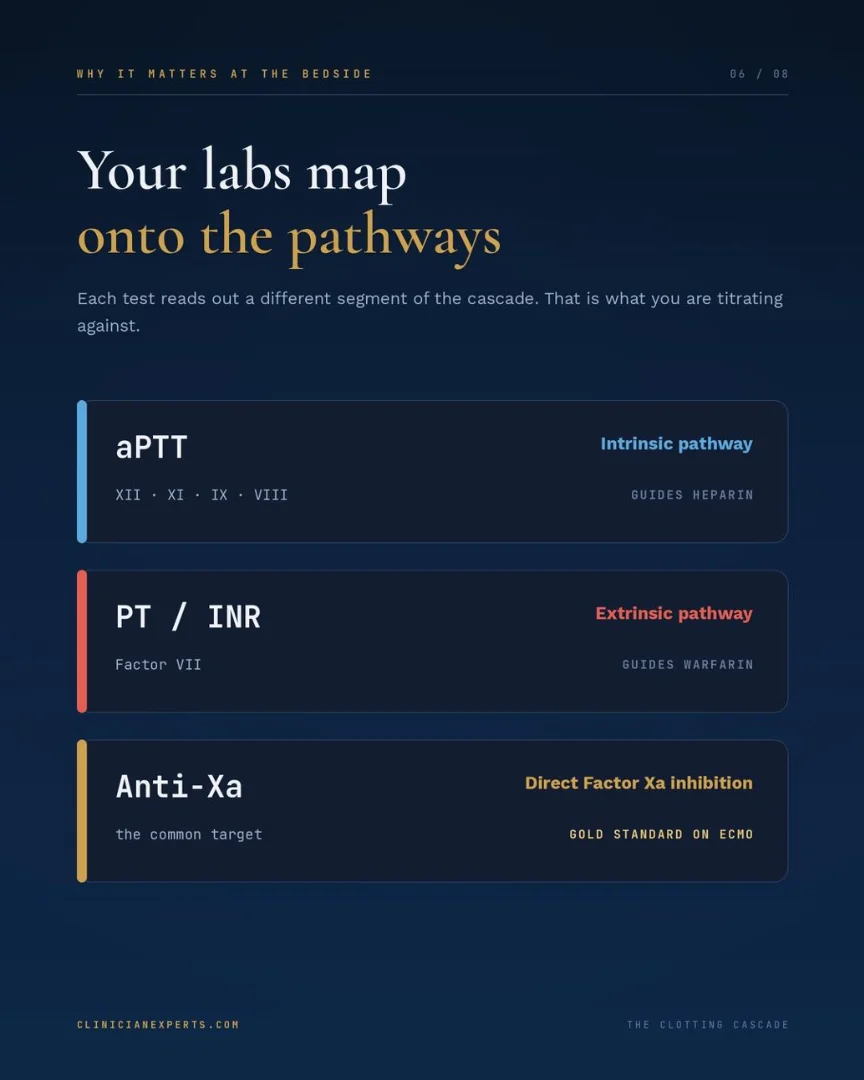
The cascade has three pathways: extrinsic, intrinsic, and common. Each one feeds into the next through a chain of clotting factors. Disrupt one factor, and the whole system can fail.
In litigation, that matters because:
- Hemophilia A means factor VIII is missing
- Hemophilia B means factor IX is missing
- Vitamin K deficiency knocks out factors II, VII, IX, and X
And then there’s antithrombin III.
AT3 is the protein that makes heparin work.
Heparin doesn’t anticoagulate on its own. It binds to AT3, and AT3 does the actual work of inhibiting clotting factors.
If AT3 levels are depleted, heparin loses its effectiveness.
The patient may look adequately anticoagulated, buttThey may not be.
In cases involving prolonged heparin use, liver disease, nephrotic syndrome, or sepsis, AT3 deficiency is a real and documented risk. It is important to have someone review the case that knows to look for the details, was AT3 checked?
Was heparin resistance investigated? Was the dose adjusted or a different agent considered?
If the answer is no, and the patient clotted or bled, that’s a problem that may a liability.
Blood thinners add another layer entirely.
Warfarin, heparin, direct oral anticoagulants like apixaban and rivaroxaban, and antiplatelet agents each carry distinct bleeding risks.
Managing them before surgery isn’t optional. It’s a clinical obligation with a timeline.
The questions I ask when doing an initial case review:
- Was the bleeding risk assessed before the procedure?
- Was anticoagulation held for the correct number of days?
- Was a bridging protocol indicated and followed?
- Was reversal considered? Was it ordered in time?
- Did the team document the decision and the rationale?
Reversal agents exist for a reason. Vitamin K and FFP for warfarin. Protamine for heparin.
Andexanet alfa for factor Xa inhibitors. Idarucizumab for dabigatran. If a patient bled out and reversal wasn’t on the table, documentation should be in place to know why.
When I review the records, I’m asking: did the team know this patient’s clotting history before surgery? Was anticoagulation managed correctly? Was a bleeding complication caught in time?
The coagulation cascade ends with fibrinogen converting to fibrin, forming a stable clot.
When that process breaks down and nobody acted on the warning signs in the chart, that’s where negligence lives.
Clinical knowledge isn’t just bedside skill. It’s the foundation of every report I write.
As an LNC, I can find this information before you find your medical expert… which I can also help you find on the platform I built that uses both AI and a 30-point algorithm to find the top 3 best scored matches at ClinicianExperts.”

Stay updated with Hemostasis Today.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
-
Jul 26, 2026, 16:26Novi Yanti Sari: When MPNs Affect the Heart
-
Jul 26, 2026, 16:21Beyond Drugs: Can Museums Become a Medical Prescription?
-
Jul 26, 2026, 14:45Sarah Giorgia Grazia Giannone: An Exciting Chapter in Gene Therapy Research
-
Jul 26, 2026, 14:21Javed Anees: Cerebral Collateral Circulation in Acute Ischemic Stroke
-
Jul 26, 2026, 14:11André Picard։ Canadian Blood Supplies Drop Sharply, Urgent Donor Appeal Issued
-
Jul 26, 2026, 13:54Lorenzo Scalia: New Review Highlights Anticoagulant Strategies for Elderly Patients With Atrial Fibrillation
-
Jul 26, 2026, 13:32Ahmed Kotb: A Practical Guide to Von Willebrand Disease
-
Jul 26, 2026, 12:42Emmanuel J Favaloro: Celebrating Excellence in Scientific Peer Review
-
Jul 26, 2026, 12:20Advancing Sickle Cell Care Through Advocacy – American Society of Hematology