
Chokri Ben Lamine: High-Yield Clinical Insights on Carfilzomib-Induced aHUS
Chokri Ben Lamine, Adult Hematology and SCT Assistant Consultant at Oncology Center of Excellence at King Faisal Specialist Hospital and Research Center, shared a post on X:
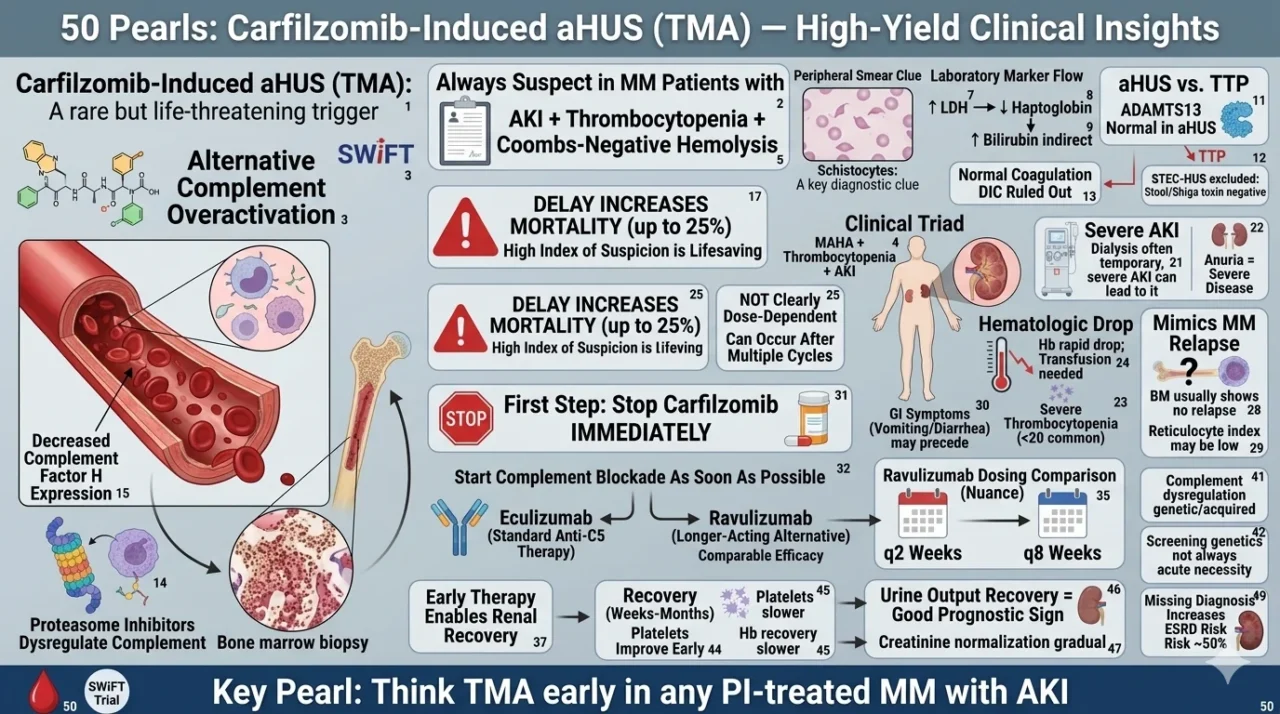
“50 Pearls: Carfilzomib-Induced aHUS (TMA) — High-Yield Clinical Insights
1.Carfilzomib is a rare but life-threatening TMA/aHUS trigger
2.Always suspect in MM pts with AKI and thrombocytopenia with hemolysis
3.aHUS is alternative complement overactivation
4.Classic triad is MAHA with thrombocytopenia and AKI
5.Coombs-negative hemolysis is key
6.Peripheral smear shows schistocytes as a diagnostic clue
7.Haptoglobin markedly decreased is strongly supportive
8. Increased LDH indicates ongoing hemolysis
9.Bilirubin indirect increases (hemolysis marker)
10.Complement levels may be normal but not reliable
11.Differentiate from TTP where ADAMTS13 normal in aHUS
12.STEC-HUS excluded with stool/Shiga toxin negative
13.DIC ruled out with normal coagulation panel
14.Proteasome inhibitors can dysregulate complement
15. Decreased Complement factor H expression is the key mechanism
16.High index of suspicion is lifesaving
17.Delay increases mortality (up to 25%)
18.Renal biopsy shows TMA features (if done)
19.Mesangiolysis with intimal edema and fibrin deposition
20.Multi-organ disease but kidney most affected
21.AKI can be severe and dialysis is often needed
22.Anuria is a severe disease marker
23.Severe thrombocytopenia common (e.g. <20)
24.Hb can drop rapidly and transfusion is needed
25.Not dose-dependent clearly
26.Can occur after multiple cycles
27.Can mimic MM relapse and be misleading
28.Bone marrow usually shows no relapse
29.Reticulocyte index may be low
30.GI symptoms (vomiting/diarrhea) may precede
31.First step is to stop carfilzomib immediately
32.Start complement blockade as soon as possible
33.Eculizumab is standard anti-C5 therapy
34.Ravulizumab is longer-acting alternative
35.Ravulizumab dosing q8 weeks vs q2 weeks
36.Comparable efficacy between both agents
37.Early therapy enables renal recovery
38.Renal recovery may take weeks–months
39.Multiple doses often required
40.Duration of therapy unclear
41.Complement dysregulation may be genetic and acquired
42.Screening genetics not always necessary acutely
43.Complement labs lack sensitivity/specificity
44.Platelets improve early with treatment
45.Hb recovery slower than platelets
46.Urine output recovery is a good prognostic sign
47.Creatinine normalization gradual
48.Dialysis often temporary
49.Missing diagnosis increases ESRD risk ~50%
50.Key pearl: Think TMA early in any PI-treated MM with AKI
Source: Opare-Addo et al., Annals of Internal Medicine Clinical Cases 2024 ”
Stay updated with Hemostasis Today.
-
Jul 9, 2026, 08:46Jordan Agay: Folate Deficiency in Patients Receiving PARP Inhibitors
-
Jul 9, 2026, 08:29Laura Katz: Is Human Lactoferrin Better Than Bovine Lactoferrin?
-
Jul 9, 2026, 08:17Anziya Sabeer: AI-Driven Non-Invasive Anemia Detection
-
Jul 9, 2026, 07:37Variable Mechanisms of ADAMTS13 Inhibition by Autoantibodies in iTTP – JTH
-
Jul 9, 2026, 07:31DHR-Sponsored Training Programme at ICMR-CRMCH Week 2 – Day 4 – ICMR-NIRBID
-
Jul 9, 2026, 06:03Barbara Adams Krolak: ISTH Launches Global Women’s Health Hub
-
Jul 9, 2026, 05:49Abdul Mannan: A Low Platelet Count is not Always a Bone Marrow Problem
-
Jul 9, 2026, 05:41Julieta Rosales: Management of Tandem Strokes – To Stent or Not to Stent?
-
Jul 8, 2026, 21:30Matthew Gouveia: How VNS-REHAB Is Transforming the Future of Stroke Rehabilitation