

Marcos Gamboa Chele: Are We Asking for Too Many Thrombophilia Panels?
Marcos Gamboa Chele, Internal Medicine Specialist, shared a post on LinkedIn about a recent article by Jiwon Shin et al, adding:
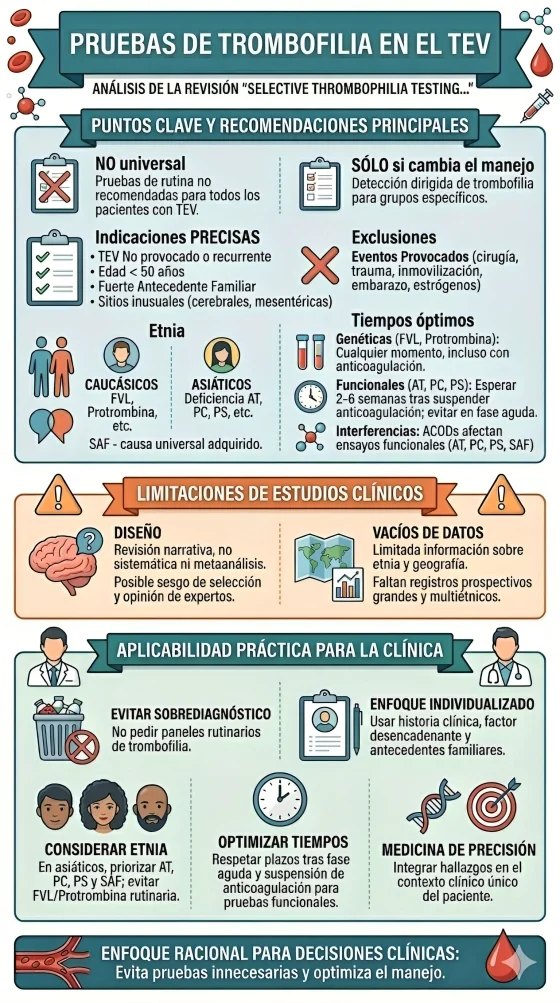
”Are we asking for too many thrombophilia panels?
Venous thromboembolism (VTE) affects 1 in 1,000 people worldwide each year. However, the current clinical evidence is clear: universal or routine screening for thrombophilia in all patients with VTE is not recommended.
Based on the recent review ‘Selective Thrombophilia Testing in Venous Thromboembolism’, here is a practical summary of its benefits, limitations, and how to apply it in our daily practice.
Benefits of Selective Testing
In carefully selected patients (unprovoked VTE, younger than 50 years, thrombosis at unusual sites, or strong family history), evaluation offers valuable information for individualized management and prevention of recurrences.
The identification of high-risk conditions, such as Antiphospholipid Syndrome (APS) or Antithrombin deficiency, may alter the choice or duration of anticoagulation, justifying indefinite therapies.
It allows for structured genetic and family counseling when serious hereditary defects are confirmed.
Limitations and Challenges
False positives and negatives: Functional assays are highly sensitive to acute phase reaction and the use of direct oral anticoagulants (DOACs), which can lead to misleading results.
Ethnic variation: Factor V Leiden and Prothrombin G20210A mutations are common in Western populations, but extremely rare in Asians. In contrast, deficiencies of natural anticoagulants are more significant in the latter populations.
Marginal clinical impact: Discovering a mild hereditary defect rarely alters the management of anticoagulation and has not been shown to improve mortality.
Practical Applicability in the Flat or Consultation
Zero tests in provoked VTE: If the event was triggered by surgery, trauma, or estrogen use, the test has limited diagnostic and therapeutic value.
Time is money: Testing for Protein C, Protein S, and Antithrombin should be postponed until the patient is recovered and 2-6 weeks after stopping blood-thinning therapy.
Lean on genetics: Unlike functional testing, genetic (DNA) testing for specific mutations can be performed at any time, as they are not affected by blood thinners or acute illness.”
Title: Selective Thrombophilia Testing in Venous Thromboembolism
Authors: Jiwon Shin, Hyejee Lee, Hyangkyoung Kim
Read the Full Article on Annals of Phlebology

Stay updated on all scientific advances with Hemostasis Today.
{kind=link}
-
Aug 11, 2026, 05:53Isaac Okello: Strengthening Sickle Cell Advocacy in Uganda
-
Aug 11, 2026, 05:38Rami Unterman: A Simple New Biomarker for Fibrotic ILDs
-
Aug 11, 2026, 04:10Haroun Gajraj: CLaCS vs Sclerotherapy – What Does the Evidence Show
-
Aug 11, 2026, 02:54Tareq Abadl: The Ultimate Guide to Clinically Significant Antibodies
-
Aug 10, 2026, 17:35Chokri Ben Lamine: Balancing Holistic Care and Precision in Hematology
-
Aug 10, 2026, 17:14Anna Stanizzi: Patient Blood Management as a New Model of Personalized Care
-
Aug 10, 2026, 17:12Odong Christopher: New Research on Ischemic Stroke Prediction in Uganda
-
Aug 10, 2026, 16:58Jeff Szer AM: Advancing the Management of Paroxysmal Nocturnal Hemoglobinuria
-
Aug 10, 2026, 16:51Suebsarn Ruksakulpiwat։ A New Milestone in the Development of the Stroke Risk Screening Scales