

Smitirupa Mishra: Early Clues Lie in Neutrophil Morphology
Smitirupa Mishra, Consultant Pathologist at Sparsh Hospitals and Lab Head at Pathkind Labs, shared a post on LinkedIn:
”Toxic Granules in Neutrophils – Practical Reporting and Clinical Relevance
Toxic granulation is not just a morphological curiosity-it is a dynamic indicator of systemic stress and marrow response, often guiding early clinical decisions.
What are Toxic Granules?
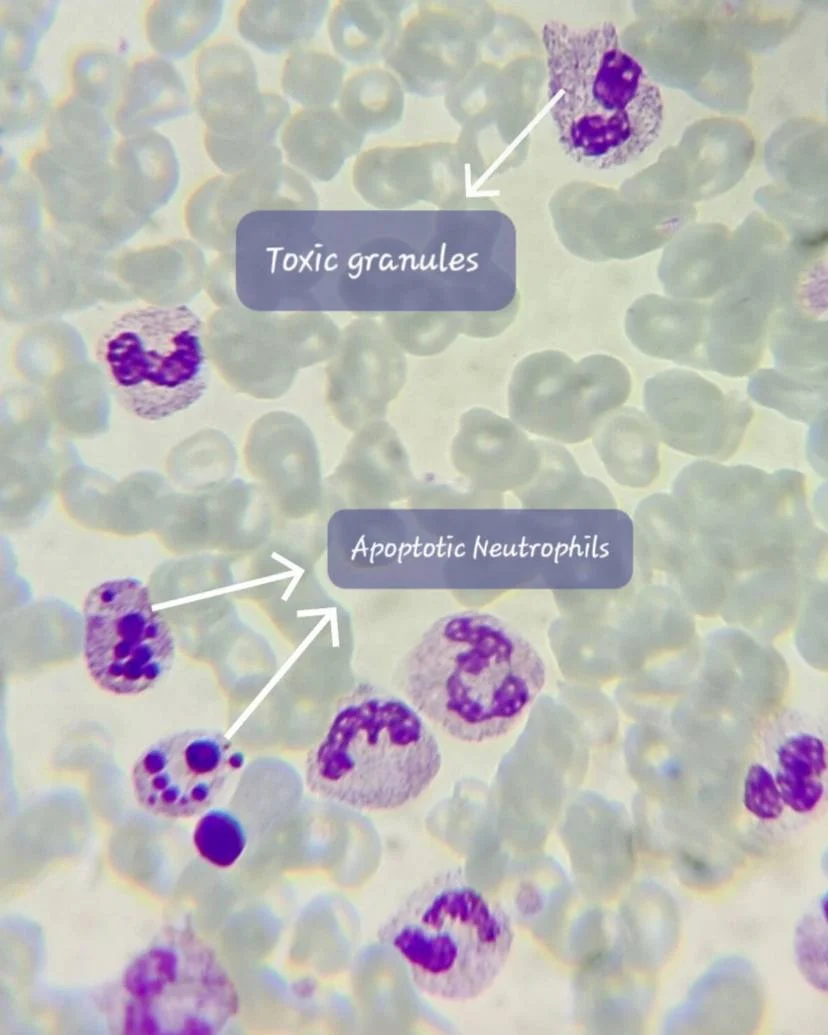
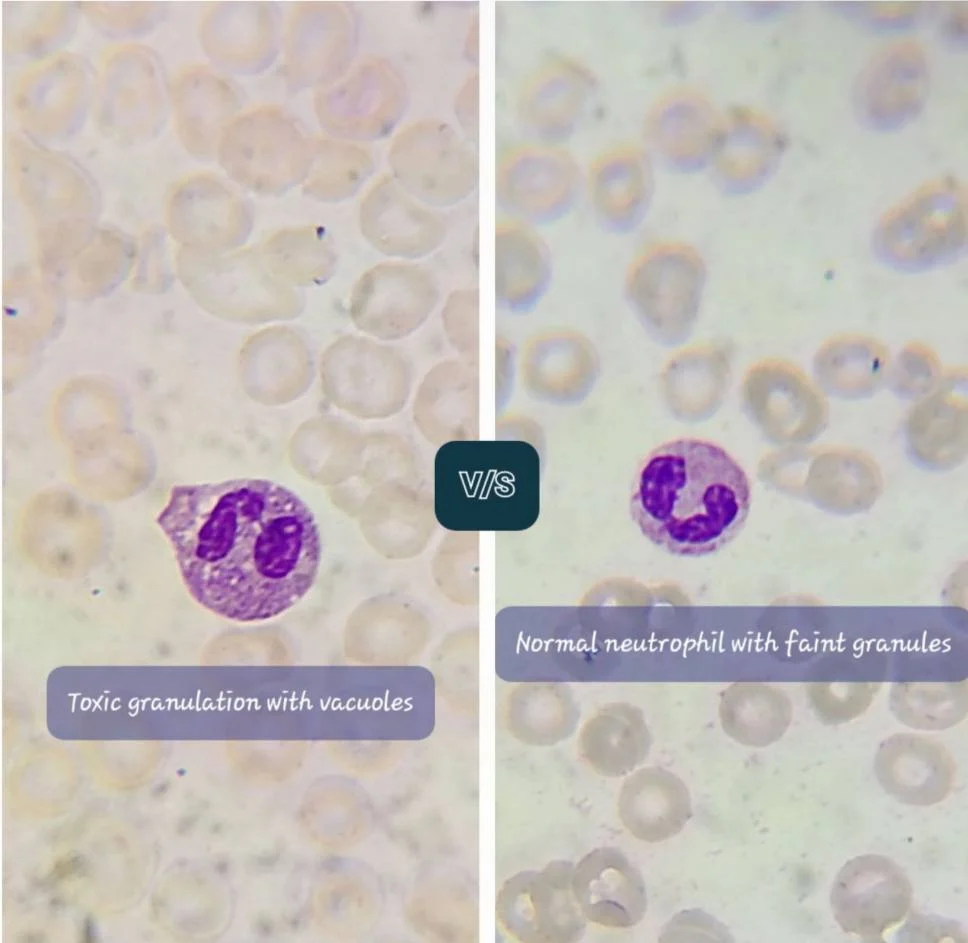
Coarse, dark blue-purple cytoplasmic granules in neutrophils representing retained primary (azurophilic) granules due to accelerated granulopoiesis under cytokine stimulation (e.g., IL-6, G-CSF).
How to Identify
Coarse, prominent, dark granules (larger than normal)
Uneven cytoplasmic distribution
Frequently associated with:
- Döhle bodies
- Cytoplasmic vacuolation
- Left shift
Always compare with internal control neutrophils on the same smear.
When Should You Report Toxic Granulation?
Based on Morphology (Primary Criterion)
Report when:
- Moderate to marked granulation
- Seen in a significant proportion of neutrophils
- Associated with other toxic changes
Should You Mention It with Normal or High WBC Counts?
Yes – WBC count does NOT limit reporting.
1. High WBC Count (Neutrophilia)
Most common scenario
Strongly supports acute bacterial infection / inflammation
Adds weight to a reactive process
2. Normal WBC Count
Very important to report
May indicate:
Early infection (before leukocytosis develops)
Localized infection
Immunocompromised states where WBC response is blunted
Toxic granulation can be an earlier and more sensitive marker than total leukocyte count.
3. Low WBC Count (Neutropenia)
If present, it is clinically significant and potentially alarming
Suggests:
Severe infection (e.g., sepsis) with marrow exhaustion
Clinical Significance
Seen in:
- Acute bacterial infections & sepsis
- Severe inflammation (burns, trauma)
- Post G-CSF therapy
- Pregnancy (mild)
What About Apoptotic Neutrophils?
How to Recognize Apoptotic Neutrophils?
Nuclear condensation (pyknosis)
Fragmentation (karyorrhexis)
Cytoplasmic shrinkage with or without vacuoles
Is there a correlation with toxic granulation?
- Toxic granulation indicates increased production and activation
- Apoptotic neutrophils indicate increased turnover and cell death
May indicate:
Intense inflammatory response with rapid neutrophil turnover
Seen in:
- Sepsis
- Severe infections
- Cytokine storm states
It reflects a high neutrophil kinetic state:
Increased production (toxic change) plus increased destruction (apoptosis)
How This Helps Clinicians
- Detect early infection, even with normal counts
- Identify severity and systemic involvement
- Distinguish reactive vs neoplastic neutrophilia
- Flag high-risk states (toxic changes plus neutropenia)
- Monitor treatment response
Pitfalls
- Don’t overcall in poorly stained smears
- Avoid reporting when minimal or focal
- Correlate with clinical context always
Take-Home Message
- Report toxic granulation based on morphology-not WBC count
- Its presence with normal or low counts is often more clinically significant
- Association with apoptotic neutrophils suggests high inflammatory turnover and severity.”

Stay updated with Hemostasis Today.
{kind=link}
{kind=link}
-
Jun 26, 2026, 18:28Daniel Pereira Monteiro: Why Is Beta Thalassaemia Major so Severe?
-
Jun 26, 2026, 18:27Pradip Pawar: Cell and Gene Therapy – Transforming Medicine in the 21st Century
-
Jun 26, 2026, 18:26Aviva Schwartz: How Can We Better Protect Patients After an Ischemic Stroke?
-
Jun 26, 2026, 18:25Does Reversing Factor Xa Inhibitors Really Carry as Much Thrombotic Risk as We Think? – RPTH Journal
-
Jun 26, 2026, 18:25Akshat Jain: Novel Therapies in Childhood Blood and Cancer Disorders
-
Jun 26, 2026, 16:57Abdul Muqtadir Abbasi: Anticoagulation in DVT Patients With Hidden Varices Requires Extreme Caution
-
Jun 26, 2026, 16:42Anesa Mulabecirovic: Why Von Willebrand Disease Takes Years to Diagnose in Women
-
Jun 26, 2026, 16:32Kaitlin Lichty: A New Identity Reflecting a Shared Legacy of Bleeding Disorders
-
Jun 26, 2026, 16:07Toong Youttananukorn: The WFH Registry Driving Better Care and Advocacy